
This Week in Birthing Stories
  November 20, 2025 Greetings, Meteor readers, Why are there so many Christmas decorations up already? Can November live!? In today’s newsletter, we look at three stories of what it’s like to seek care in America. Plus, some weekend plans. Slow it down, Shannon Melero  WHAT'S GOING ONA recurring pattern: This week, you may have seen a viral video of Kiara Manuel, a woman in active labor at Dallas Regional Medical Center, having to answer intake questions while screaming in pain. Her mother, who recorded the ordeal, told local news outlets that staff at the hospital had left Manuel without care for over half an hour, choosing “paperwork over life.” This week, you may have seen another viral video of Mercedes Wells, a woman who was told by a hospital in Indiana that she wasn’t really in active labor and was sent away. Eight minutes into her drive home, she gave birth on the side of the road. Wells’ sister-in-law told ABC 7 Chicago, “Mercedes begged her,” referring to a nurse. “She really begged her, she said I can feel it, I’m in active labor. She just ignored her.” This week, you may have read the story of Tierra Walker, a mother in Texas who asked for an abortion after her pregnancy had left her “wracked by unexplained seizures” and at high risk for preeclampsia. Doctors at Methodist Hospital Northeast near San Antonio told Walker that under the state’s ban, they could not abort because there was no emergency—her pregnancy was fine, it was only her health in trouble, according to ProPublica, which broke the story. Walker’s son found her dead a month later, killed by preeclampsia. All three of these women have one thing in common: they were Black women seeking reproductive care in America. It is a well-known statistic that maternal mortality rates among Black women are more than double that of any other racial group in the United States. Even outside of giving birth, Black women seeking care for any health issues face an onslaught of discrimination and neglect, rooted in centuries of racism. One would assume that, given the staggering statistics, more would have been done to address the issue. But the stories of Kiara, Mercedes, and Tiara show us that it remains persistent, entrenched, and lethal—even though we know much of what it would take to improve Black maternal health. In the last two years, legislators have introduced the Black Maternal Health Momnibus Package and the “MOMMIES” Act. The Momnibus has seen some success in inspiring similar state laws, like this one in Michigan that recognizes and makes illegal “obstetric racism” and “obstetric violence.” But neither Momnibus nor the MOMMIES Act (which focuses on expanding Medicaid coverage for those who give birth) has received enough support from Congress to be passed. So why aren’t we all doing more? Well, that is the incredible hold that systemic racism has on every aspect of this country. Despite the valiant attempts of some advocates in Congress, most members have not prioritized the issue. And even if they did, the issue requires holistic, aggressive approaches to even slightly move the needle in the right direction: racial bias training, new pathways to increase the number of Black OB-GYNs, accessible midwifery care, updated postpartum care and leave policies, and research funding to understand these disparities and the health conditions (like preeclampsia) that are more prevalent among Black women—and that’s just the beginning. But it’s worth tackling. The business of birthing intersects with nearly every facet of life, from education to economics to infrastructure, and until it is treated as such, we will continue living in a world of too many viral videos, and too little action. AND:
  “The Most Important Event Nobody Knows About”
It happened 48 years ago this week, in HoustonBY EMILY KOH  CORETTA SCOTT KING AND FELLOW DELEGATES AT THE 1977 NATIONAL WOMEN'S CONFERENCE. (VIA GETTY IMAGES) Forty-eight years ago this week, my grandmother, Dr. Hesung Chun Koh, joined thousands of women from around the world in Houston, Texas to make history. They came to the first—and only—National Women’s Conference to adopt a National Plan of Action to improve the status of women in America. The plan delegates ultimately adopted at the conference included recommendations on a range of issues—including child care, education, health, and reproductive freedom—that still impact the lives of women today. The conference brought together women from all walks of life, from leading figures including Coretta Scott King, Maya Angelou, and First Ladies Rosalynn Carter, Betty Ford, and Lady Bird Johnson to working women, “homemakers,” and students. It was a historic milestone in the women’s movement and American history, yet its impact is overlooked. Reflecting on the conference, Gloria Steinem declared it “a constitutional convention for the female half of the country.” And she noted: “It may take the prize as the most important event nobody knows about.” It’s time to change that. The conference was an inflection point: a pinnacle achievement for the women’s movement. It also spurred backlash: Opponents who protested it pushed back on the idea that women deserve a full and equal role in public life. Now, that backlash remains as fierce as ever before, and our movement is at another inflection point. We are rapidly losing decades of progress; America is devolving into a nation where women are second-class citizens, transgender and nonbinary individuals cannot live openly and safely, and men suffer from rigid expectations of masculinity. In two years, the fiftieth anniversary of the 1977 National Women’s Conference will be here—and a chance to revisit the National Plan of Action and co-create a new vision with women from all walks of life, men, and the LGBTQ+ community. My grandmother immigrated to America from Seoul, South Korea, for college, and became one of the first Korean women to earn a doctorate in the United States. Her focus on the future made my life possible and created opportunities for the next generation. The vision she and her fellow delegates set forth in Houston can inform and inspire our work today. The question before us now is the same one they faced then: Will gender equity and equality advance or fall backwards in our lifetime? History calls on us to move forward. Emily Koh served on the White House Gender Policy Council in the Biden-Harris Administration. She is currently working on an initiative to advance gender equity and equality in the U.S. that centers on the 50th anniversary of the 1977 National Women’s Conference.  WEEKEND READING 📚On screen: Parents, it might be time to free yourself from YouTube Kids. (The Verge) On a special kind of wellness: Orgasm. Cult. (TCF Emails) On the state of men: Apparently, some men are searching for the tough love they desire in…the Orthodox church? (Yes, of course “traditional values” are part of the pitch.) (The New York Times)  FOLLOW THE METEOR Thank you for reading The Meteor! Got this from a friend? |
Does RFK Jr. Know the Scientific Method?
 September 22, 2025 Greetings, Meteor readers, We are closed tomorrow in observance of Rosh Hashanah, but we couldn’t let you go into the week without your favorite newsletter! But before we take a little rest, let’s talk about Tylenol. Raw dogging our headaches, Shannon and Mattie  WHAT'S GOING ONFor the past two weeks, news has been swirling that the Department of Health and Human Services is expected to announce a potential link between pregnant people’s use of Tylenol and a supposed increased risk of autism in children. Those reports intensified over the weekend, and senior officials are now briefing media outlets on background. The timing makes perfect sense for exactly one person and no one else: That would be HHS Secretary Robert F. Kennedy Jr. Yes, the same man who is imperiling millions of children with his documented anti-vaccine agenda and has admitted to having a literal brain worm. Several months ago, he said that he intended to find the root causes of autism before the end of September. With October on the horizon, he must be feeling the pressure. So here we are. The expected new guidance—which is expected to drop before the end of the week—will tell pregnant women not to use Tylenol except in cases of high fevers, robbing them of one of the few options they have to manage pain for the 40 weeks they spend growing another human. (Doctors have long recommended Tylenol, the name brand for the generic acetaminophen, because similar fever reducers and pain relievers like Ibuprofen, the generic drug behind Advil, have a documented association with miscarriage and potential fetal harm.) The obvious question, of course: Is Tylenol dangerous? While some limited research has suggested a possible association between Tylenol consumption and autism, larger studies—including a recent and major examination of the outcomes of 2.5 million children in Sweden—have turned up no connection. And the American College of Obstetricians and Gynecologists recently affirmed the recommendation of Tylenol in a recent statement to CBS News, telling the outlet that “there is no clear evidence that proves a direct relationship between the prudent use of acetaminophen during pregnancy and fetal developmental issues.” The prevalence of autism has increased over the past 25 years, according to CDC statistics, with a range of possible explanations. One that we know to be true is that the definition for what constitutes the condition has changed and expanded, making it easier to be diagnosed (and to access services). What we also know to be true? The drug Tylenol has been available over the counter for almost 70 years—well before the documented growth in cases. So scientists, researchers, and those who can count agree: Tylenol is not the likeliest culprit for the increase in autism rates. They reach that conclusion via the scientific method, which isn’t just a unit in high school curricula. It’s an actual process that actual scientists respect. It involves investigating observable phenomena through rigorous testing and careful experimentation. It does not involve setting self-imposed deadlines and drumming up questionable research to meet them. But there is no doubt that this announcement will confuse pregnant women, their providers, and their families. It will, in all likelihood, make those who are experiencing pain while pregnant (that’s 100% of pregnant people, FYI) hesitate before treating it, wondering if their degree of discomfort justifies a dose of relief. (Even though we know that stress and pain can themselves lead to adverse outcomes for babies, including preterm birth, low birth weight, high blood pressure, and other complications.) This announcement will not make pregnant women or children safer or healthier, but it will sow more doubt in the medical establishment, and it will make women suffer. — Mattie Kahn AND:
 I BELIEVE THIS IS WHAT THE YOUNG PEOPLE CALL AURA. (VIA GETTY IMAGES)
 FOLLOW THE METEOR Thank you for reading The Meteor! Got this from a friend? |

"They're Sacrificing Our Children"
 September 4, 2025 Salutations, Meteor readers, There will be no news today, as I’ve instead chosen to use this time to send a second-by-second reaction essay to the trailer for Emerald Fennell’s Wuthering Heights. Kidding! In today’s totally normal newsletter, we learn about how we’re currently living in a Planet of the Apes prequel. Plus, author Scarlett Harris on the significance of Mariah Carey receiving the Video Vanguard Award (her first VMA) this weekend. Shannon Melero  WHAT'S GOING ON“There’s no precedent for this”: Yesterday, Florida’s surgeon general announced that the state plans to end all vaccine mandates for everyone, including schoolchildren. That means that the long-time, lifesaving vaccines for polio, measles, and many more (very! preventable!) diseases could become options rather than requirements. I had one obvious question: what the fuck? So I spoke to Dr. Dara Kass, an emergency room physician and healthcare policy consultant in New York. “To be clear, they’re not banning vaccines,” Dr. Kass clarifies. “They're saying your pediatrician may not stock it, your insurance may not cover it, [and] the other kids in school may not be vaccinated.” And without a requirement in place, insurance companies get the message that they don’t have to cover these treatments, making it more difficult for them to be readily available at doctors’ offices and pharmacies. Suddenly, the burden shifts to the consumer, and if there’s one thing American consumers know, it’s that our for-profit insurance companies will do what is in the interest of their bottom line, not public safety (because it’s literally not their job). In other words, Dr. Kass explains, elected officials are working to “make [vaccines] much harder for us to get, and they didn’t advertise that when they went into office.” It would appear that Florida is taking advantage of a chaotic moment in federal vaccine guidance, but Dr. Kass disagrees. “I think that this is a long-standing plan that [the Florida GOP] have to be inflammatory and extremist,” she argues. “The lack of leadership at HHS is empowering Florida to do things that are the most inflammatory and the most extreme. No rational person thinks that dismantling requirements for schoolchildren—which helps community safety—is a logical and smart idea.” Dr. Kass says that officials like Florida Surgeon General Joseph Ladapo are “sacrificing our children” to prove they’re in alignment with Robert F. Kennedy’s leadership and the MAHA agenda to “dismantle our public health infrastructure.” “This is clearly an attempt to do that,” she says. “There's no precedent for the idea of removing requirements for vaccines for anybody.” And it isn’t just a Florida problem. Imagine, if you will, unvaccinated children who unknowingly have a virus in their system running around sneezing on everything as children are wont to do—and coming into contact with the elderly, with the immunocompromised, with people suffering from long covid. Adults who fall into those categories, vaccinated or not, will be affected by these changes because, as Dr. Kass explains, “older Americans rely on herd immunity” for protection. You don’t have to work too hard to picture the worst-case scenario because there is an entire film genre dedicated to painting that picture. (See: the entire Planet of the Apes franchise, Contagion, I Am Legend, or any zombie movie ever.) It’s not all negative, though. States like Pennsylvania, California, Washington, and Oregon are reacting to the federal government abandoning the ship of public health by actually being helpful. Pennsylvania announced that its vaccine policies will be guided by (you’ll never believe it) the top medical societies in the state. Meanwhile, the three western states are combining forces to create the West Coast Health Alliance to “uphold scientific integrity in public health.” So, as we always like to say when things start to go completely off the rails: call your representatives, no matter their party. One thing we should all be able to agree on is that more people dying from preventable illnesses is bad, and the only way to move forward is with proven, effective science, which we have! Ask your representatives to commit to following the science and not the changing winds of political power. And if they’re reluctant to speak up, just remind them that every person who dies—and people will die if this becomes the norm—is one less vote for their re-election. That’ll get their attention. AND:
 BY SCARLET HARRIS Why Mariah's First Moonman Matters MARIAH AT THIS YEAR'S BET AWARDS (VIA GETTY IMAGES) This weekend at the MTV Video Music Awards, Mariah Carey is being awarded the Video Vanguard Award—her first VMA. If it feels long overdue, that’s because it is. While the Songwriters Hall of Fame inducted Mariah in 2020, her videos have, until now, gone unrecognized at the biggest industry awards show. That oversight is especially galling, given that Mariah—a powerhouse biracial woman with a vocal range that could shatter glass—has understood the power and impact that a video can have since the start of her career. Long before the idea of women musicians controlling their own image and voice went mainstream, Mariah directed several of her earliest and most influential videos, from the deceptively simple “Fantasy” (’95, with that iconic fairground clip to “Always Be My Baby” (’97) to the Life of a Showgirl-coded “Breakdown” (’97). “I’d done a lot of videos and wasn't always a hundred percent thrilled,” she said at the time. “So I figured I would give directing a shot.” It worked. The Mariah-directed videos reflect a gaze that actually centers her face—a novel idea at the time.  BACKSTAGE WITH LL COOL J AT THE 1997 MTV VIDEO MUSIC AWARDS (VIA GETTY IMAGES) With her remixes, which were often given more attention than the original tracks, Mariah became a reverse crossover star—from pop into R’n’B. No mean feat as Mariah was famously under the thumb of her controlling husband and manager, record executive Tommy Mottola, who was intent on continuing to market her as the girl next door instead of letting her explore her biracial identity and R’n’B roots. In 2022, when Pitchfork’s then-editor-in-chief Puja Patel named the “Fantasy” remix featuring Ol’ Dirty Bastard the best song of the 1990s, shåe lauded the track as “a declaration of independence, a reclamation of agency and identity, a blueprint for a new kind of pop song that would be replicated for decades to come.” (Certain men were very, very mad about that.) Mariah’s musical career had highs and lows after that: Glitter was panned; The Emancipation of Mimi was triumphant, and since then, Mariah has shot videos that are self-referential (“Touch My Body,” ’09), audacious (the Eminem diss track “Obsessed,” ’09), and more. But all the while, she has wielded absolute control over her image, including as the reigning, ageless Queen of Christmas. (It’s nearing that time…) Today, her influence is felt in the world-building that Beyoncé and Taylor Swift offer in their visuals. And like Beyoncé, who only picked up a Grammy for Album of the Year this year, Mariah is a woman of color who has been overlooked too long. She has five Grammys in genre categories, but she’s never won the big one, calling the awards show “overrated.” It speaks to the outsized impact women of color, and particularly Black women, have on culture—while simultaneously being snubbed by the establishment. Now Mariah is finally being awarded her due. Rock & Roll Hall of Fame, your move.  Scarlett Harris is a culture critic, author of A Diva Was a Female Version of a Wrestler: An Abbreviated Herstory of World Wrestling Entertainment, and editor of The Women Of Jenji Kohan.  FOLLOW THE METEOR Thank you for reading The Meteor! Got this from a friend? |

Can Mifepristone Help Prevent Breast Cancer?
 August 19, 2025 Top of the evening, Meteor readers, Anyone else lose half their day binging the first set of Love is Blind UK episodes? No? Just us? Oh, well! In today’s newsletter, we take a look at a new way scientific research is being hindered by political ideology. Plus, a sleepover for one at the Texas House. Love innit, The Meteor Team  WHAT'S GOING ONSlowing down science: Earlier this month, when Health and Human Services Secretary Robert F. Kennedy Jr. announced the cancellation of some mRNA vaccine research, we wrote about the devastating toll that move could have on breast cancer research specifically. But it turns out that’s not the only hit breast cancer research is taking. Last week, a group of reproductive health experts published an opinion piece in the medical journal The Lancet, drawing attention to the potential that the drug mifepristone—best known as an “abortion pill”— could also be used as a tool to prevent breast cancer in high-risk patients. There’s just a bit of a roadbump: Because of the extensive “regulatory, political, and legal barriers” around the drug, the experts fear that researchers and pharmaceutical companies are failing to invest in exploring mifepristone’s possible benefits. As one of the piece’s authors, Kristina Gemzell Danielsson, writes, “We have very promising data, but no efforts are being made to continue with the research…the regulatory hurdles are absurd, probably because [mifepristone] is associated with induced abortion.” The writers of The Lancet come from all over the world, but their concerns have particular resonance in the United States, where more than half of the states have some sort of restriction on mifepristone, and on a federal level, RFK Jr. has asked the FDA to review mifepristone again, claiming safety concerns. To be clear: the drug is well-researched and has also been deemed safe and effective in nearly 100 countries. The development of new treatment options for BRCA1- and BRCA2-positive patients is urgent. People with those gene mutations have a significantly elevated lifetime risk of developing certain cancers, including breast cancer, and for now, the most common treatments recommended to them are prophylactic double mastectomies and hysterectomies. These surgeries are invasive and emotionally taxing, plus, they don’t fully guarantee remaining cancer-free. According to The Lancet, some preliminary studies have shown that mifepristone could curb progesterone, the hormone that drives the kind of uncontrolled cell growth that is a hallmark of cancer. While there still have not been clinical trials to prove the efficacy of mifepristone as a form of preventative treatment, the possibility that a pill could replace a massive, life-altering surgery is worth every penny of investment. So what can be done? The researchers behind The Lancet editorial are asking political leaders to remove the barriers and collaborate on accelerated research to study utilizing mifepristone—a drug that, again, we already know is incredibly safe. “Ideology can slow everything down,” Danielsson writes. We’d hope that even the GOP could admit that making progress on breast cancer research is an area for common ground. The Meteor reached out to the Department of Health and Human Services to ask whether it supports new research into potential uses for mifepristone and, if so, how it plans to make the drug available to researchers when over a dozen states have banned its use. Representatives from the department have not responded to our request for comment. AND: 
 SCREENSHOT VIA INSTAGRAM
 FOLLOW THE METEOR Thank you for reading The Meteor! Got this from a friend? |

A "Devastating" Blow to Breast Cancer Research
  August 7, 2025 Another green dildo was thrown onto a WNBA court last night, this time hitting two spectators and the Fever’s Sophie Cunningham. It’s the third dildoing in less than a month, and frankly, it’s the dumbest. We’ve all seen Cunningham yoke a girl for less, and some young punk really thought she was the one to try? In today’s newsletter, we take a look at RFK Jr’s latest chicanery. Plus, we take a quick trip to Love Island with Julianne Escobedo Shepherd to learn about colorism. We’ve also got your weekend reading list. Staying on Sophie’s good side, Shannon Melero  A “tremendous” setback: This week, known vaccine hater Robert F. Kennedy Jr. announced that the government would be canceling roughly $500 million in contracts committed to the development of mRNA technology—the research responsible for making viable COVID vaccines and saving millions of lives. Scientists have long been studying other applications for mRNA technology, looking to develop better flu vaccines and studying the possibility of putting mRNA to work in treating melanoma, lung, and pancreatic cancers. With some early success in those areas, hope was starting to bloom that mRNA technology could potentially improve women’s health in particular, via new ways to treat and even prevent breast cancer—but when it comes to medical research, hope dies without dollars. “The attacks on vaccine research are devastating to the future of breast cancer research,” Fran Visco tells The Meteor. Visco is the president of the National Breast Cancer Coalition and a 30-year breast cancer survivor. “We're just beginning to look at vaccines as possible treatment and prevention for breast cancer, and having the head of the Department of Health and Human Services say that mRNA vaccines have safety issues and pulling vaccine research funding…is going to set back breast cancer research tremendously,” she says. Essentially, the federal government has removed a tool in the fight against breast cancer before researchers have really even had the time to learn if it’s useful or not. Such a short-sighted move, Visco believes, means scientists won’t have the means to investigate what mRNA is fully capable of, because the government is the largest supporter of biomedical research in the country. There’s also a concern that the public may become more skeptical of vaccine research as a whole. “You need the public to believe in [the safety of mRNA technology] because they're going to have to enroll in the clinical trials in order to test whether these vaccines are effective or not,” Visco explains. “If the public is getting the message that the federal government doesn't believe in it, they will not want to be engaged in that type of research…so it hurts you at every level, and there's absolutely no basis for what the federal government is doing right now in terms of vaccines.” A number of medical researchers have called these funding cuts dangerous and argue that the decision flies in the face of decades of established scientific research. Visco echoes their concerns and cuts straight to the point: “People are going to die because of the positions that this administration has taken in health and research.” AND:
 The Call is Coming From Inside the VillaLove Island: USA has Latine viewers confronting their anti-Black historyBY JULIANNE ESCOBEDO SHEPHERD  MEMBERS OF THE SEASON 6 CAST AT AN EVENT IN NEW YORK (VIA GETTY IMAGES) Love Island is the escapist watch of the summer with its outsized personalities and tropical setting—but as the aftermath of this season has proven, it’s never truly an escape from the dynamics of the real world. A little background if you’re not one of the tens (hundreds?) of millions that made this season Peacock’s biggest streaming series ever: Love Island is a reality show in which a dozen “sexy singles” are sequestered inside a neon villa with the sole directive to find love amongst themselves, has been airing for a decade in the UK, and six years in the U.S., but it didn’t really take off here until last year, thanks to improved production values after a switch from CBS to Peacock. This summer, it was an inescapable hit: Love Island seemed like the only thing unifying the country, to be honest, a fact I chalked up to our desperate collective need for an hour of reprieve from encroaching fascism. And since it airs almost every single day for two months, it’s easy to immerse oneself in the petty dramas and flirtations of its sculpted and spray-tanned twenty-something cast. I’ve been watching Love Island for years—last summer I realized I had seen over 550 episodes, at which point I had to stop counting—and like the best reality shows, it manages to put larger-world concerns under a microscope; its anthropological utility is vast. Even in its unreal Fijian (or Mallorcan) setting, familiar biases and prejudices play out in real time. And this year especially, anti-Black racism has shown up both in the villa and among the show’s fanbase. This year was notable for the way Olandria Carthen and Chelley Bissainthe, this season’s beloved Black women leads, were characterized by fans and certain tabloid media. They were both perfectly dignified and two of the main reasons the season was watchable—only to find that, having emerged from the villa at the end of the season, they’d been saddled with the “angry Black women” stereotype. (Production has also been accused of airing decontextualized outbursts by Huda Mustafa, Love Island’s first-ever Palestinian cast member and an outspoken mother, while editing out the male behavior that led to her outbursts.)  WEEKEND READING 📚On resisting fascism: Meteor collective member Sarah Sophie Flicker tells the history of the Danish resistance—including her own great-grandfather’s role in it—and reminds us that we too can say no to tyrants. (The Nation) On ridesharing: “Uber received a report of sexual assault or sexual misconduct in the United States almost every eight minutes on average between 2017 and 2022.” The worst sentence you’ve ever read. (The New York Times) On your face: Wedding cakes are meant to be eaten, not shoved up the bride’s nostrils. Don’t marry these men! (The Cut)  FOLLOW THE METEOR Thank you for reading The Meteor! Got this from a friend? |
Postpartum Depression is a "Gift"
  July 24, 2025 Howdy, Meteor readers, I spent half my day in the waiting room of an auto shop watching reruns of Law & Order: Special Victims Unit. The things Olivia Benson has been through are insane; no wonder this show is such effective copaganda.  In today’s newsletter, we’ve got babies on the brain. Nona Willis Aronowitz, whose own baby is due any day now, explains the latest MAHA tomfoolery on postpartum depression and then asks three very important questions about baby sleep. Shannon Melero  WHAT'S GOING ONMAHA targets mamas: Earlier this week, an FDA panel discussing the use of selective serotonin reuptake inhibitors (SSRIs) during pregnancy made waves in the medical community–and not the good kind. It was so chock-full of misinformation and “MAHA talking points” that the American College of Obstetricians and Gynecologists (ACOG) felt compelled to put out a statement calling the panel “alarmingly unbalanced” and accusing it of ignoring “the harms of untreated perinatal [before, during, and after birth] mood disorders in pregnancy.” A quick review of the accepted scientific facts here: Postpartum depression affects one in eight women; mental health conditions, including suicides and overdoses, are a leading cause of death in pregnant women; and maternal mental health has taken a nosedive in the last few years. Meanwhile, there’s medical consensus that the small risks of taking SSRIs during pregnancy are far outweighed by the serious risks of untreated depression. Yet the vast majority of panel participants repeated widely debunked lies about the dangers of taking SSRIs while pregnant, claiming that the medications pose an increased risk of autism (they don’t), as well as preterm birth, pre-eclampsia, and postpartum hemorrhage (the effects are negligible). Even more enragingly, as Mother Jones’ Julianne McShane pointed out, several of these “experts” seemed to deny the gravity and even existence of the reason many patients might choose antidepressants to begin with: perinatal depression itself. Dr. Roger McFillin, a psychologist and anti-vaccine advocate, suggested that women are “naturally experiencing their emotions more intensely, and those are gifts,” not “symptoms of a disease.” FDA Chief Dr. Martin Makary opted to discuss the “root causes” of perinatal depression, like the lack of “healthy relationships” and “natural light exposure,” rather than the immediate solutions patients need. And a third male panelist, Dr. Josef Witt-Doerring, who runs a clinic that helps people wean off psychiatric medications, claimed that symptoms of depression “are not things to be fixed with medical intervention.” As a very pregnant person who’s intimately aware of the havoc hormones can wreak, these words make my blood boil–no, incinerate. With my first child, I had clinical anxiety, both during and after my pregnancy. It cost me a lot: sleep, relaxation, closeness with my partner, peace with my baby. I’m a white, educated woman who’s squarely in the demographic of people who take SSRIs most frequently, yet the stigma was still too strong for me to seriously consider the drugs. I gutted it out for far too long, and it was tough to claw my way back. But halfway through this pregnancy, as the memory of those dark times loomed, I gingerly asked my midwife whether she thought a low dose of SSRIs would prevent a disastrous redo. It was only after she reassured me it was safe and effective, sending me links to several studies, that I started taking a prophylactic dose of Zoloft in preparation for birth. Among the FDA panel’s proposed solutions was to slap a black-box warning about the use of SSRIs during pregnancy. This kind of warning might very well have deterred me–someone with a lot of access to information. I can only imagine how many more suffering women it could discourage. Like many issues the MAHA movement focuses on, this one dovetails with legitimate concerns about the overprescribing of SSRIs and the lack of holistic support for people struggling with their mental health. Those are real problems. But steering new moms away from evidence-based help can only lead to harm. “So many women I see feel guilty about taking medications,” Dr. Nancy Byatt, a perinatal psychiatrist at the UMass Chan Medical School, told The New York Times after she watched the FDA panel. “They think they should ignore their needs for their babies. And I think it could make their decisions a lot harder … because it could cause unnecessary alarm.” The Department of Health and Human Services has refused to comment on future policy decisions, but in the meantime, you can still get accurate pregnancy information from ACOG and the Society for Maternal-Fetal Medicine. —Nona Willis Aronowitz AND:
 WHAT ALL THE AI CHATBOTS ARE GOING TO START SOUNDING LIKE ONCE THEY BECOME UNWOKED.
 THE UNINSURED ICON. (VIA GETTY IMAGES)
 Three Questions About...Baby SleepWe spoke with Dr. Harvey Karp, inventor of the SNOO, about soothing the ills of modern parenthood.BY NONA WILLIS ARONOWITZ  DR. KARP, BABY WHISPERER. (VIA GETTY IMAGES) Whether or not you know Dr. Harvey Karp by name, you’ve probably absorbed his influence on baby sleep and soothing. The resurgence of the swaddle? The ubiquity of white noise in babies’ rooms? Cribbed (no pun intended) from Dr. Karp’s bestselling book The Happiest Baby on the Block. And he’s probably best known for SNOO, a pricey “smart bassinet” that rocks and jiggles a strapped-in baby all night long. In my ninth month of pregnancy, I spoke with Dr. Karp about the evolution of his signature product, what nuclear families are missing, and why sleep is a feminist issue. When SNOO first came out in 2016, it was a signifier of luxury–Beyoncé and Jay Z reportedly owned several. Now, it’s used in hospitals, including to soothe babies who were born dependent on opiates, and you’re working to have SNOO covered by Medicaid. That seems like quite a shift–how did that come about? Yes, SNOO was really known as this bougie baby bed in the beginning, but the goal was always to make it accessible to everyone. We built the bed to be reused over and over again. It’s sort of the way breast pumps started out: There were these industrial breast pumps and they were too expensive for people to buy, but you could rent them. And so, our goal was always to have SNOO be either rented or for free, and not to be purchased and owned. We have a project going on in Wisconsin right now, where hundreds of [SNOOs] are being given to families who have premature infants, mostly Medicaid recipients. Our job is to develop the science to convince Medicaid payers that we can save money and improve outcomes. We’ve also had a lot of success with companies offering SNOO as an employee benefit. Now, tens of thousands of people get a free SNOO rental from their employer, from big companies like Dunkin' Donuts to the largest duck farm in America. You often say that SNOO can help replenish what we’ve lost in terms of the extended family and support for new parents. But I think some people still feel a little funny about swapping out human cuddles for a machine. What do you say to that? Yes, a hundred years ago, and for the entire history of humanity, we had extended families, and people lived right next door to their grandmother, their aunt, their sister, and everybody shared the work. Then we moved to the city or moved hours away from our family, and women got more work responsibilities outside the home. This became pretty crushing on parents, especially single parents. So the SNOO goal is to be a helper. It's there in the home when you're cooking dinner, when you’re taking a shower, when you're playing with your three-year-old, when you are getting some sleep. It’s not set it and forget it, but it can give you 20 to 30 minutes here and there, as well as giving an extra hour or even up to two hours of extra sleep. In the womb, the baby is being held 24/7. Then they’re born, and 12 hours a day we put them in a dark quiet room. That’s sensory deprivation compared to what they had before they were born. So why, because you only have a few people in your family, should the baby miss out? SNOO…doesn’t replace what the parents would be doing, because no one can rock them all night long. It just gives the baby a little extra. When I had my first baby, sleep was a locus of inequality in my relationship–my male partner was obviously getting more of it, especially because I was riddled with anxiety about whether my baby was safe. Sleep became a feminist issue in my mind. How do you see SNOO responding to these gender dynamics, which seem to be common? We’ve definitely moved in the direction of gender equality, but we’re still far from it. Even when the baby is sleeping, sometimes moms are awake and anxious knowing that they have to get up in three hours. SNOO can help with that: There have been studies reporting that SNOO reduces maternal depression and maternal stress. There are five things that trigger depression and anxiety that SNOO improves: up to 41 minutes more sleep for mothers per night, reduced infant crying, less anxiety that the baby is in danger, the feeling that you have a support system, and [the fact that it] makes you feel like you’ve gotten things managed better. Also, men very often take on the role of being the sleep experts when they have a SNOO in the house. Men want to manage this gadget. That takes a burden off the shoulders of the mom. This conversation was made possible by Happiest Baby, a sponsor of UNDISTRACTED with Brittany Packnett Cunningham.  WEEKEND READING 📚On the boys: Everyone’s worried about young men, but are we maybe blowing the “boy crisis” out of proportion? (The New York Times) On boobs: We’re all thinking about them. And apparently so is American Eagle. (TCF Emails) On the genius invested in women’s sports: The WNBA is in the midst of negotiations for a better bargaining agreement. They’ve got a Nobel Laureate in Economic Sciences on their side. (Sports Illustrated)  FOLLOW THE METEOR Thank you for reading The Meteor! Got this from a friend? |

An "Unwed" Woman Denied Prenatal Care
  July 23, 2025 Greetings, Meteor readers, Some personal news: Stevie Nicks and Lindsey Buckingham announced a reissue of Buckingham Nicks in the middle of Mercury retrograde in Leo, and I have been UNWELL all day. Making up with your ex during the celestial season of exes resurfacing?? Stevie, the white witch that you are!  In earthly news, we take a look at an unbelievable story out of Tennessee. Plus, the continuation of the one scandal to rule them all. Your silver spring, Shannon Melero  WHAT'S GOING ONMawwaige is necessawy: Thanks to the efforts of conservatives in Tennessee, a woman with a wanted pregnancy was denied prenatal care on the grounds that her “unwed” status was in conflict with a medical provider's religious beliefs. No, this is not a throwback anecdote from the ‘50s, a time when unwed women couldn’t get birth control or credit cards. This occurred just weeks ago. It was enabled by Tennessee’s new Medical Ethics Defense Act, passed in April, which allows medical providers to deny care based on their religious, ethical, or moral beliefs. At the time, Nona Willis Aronowitz identified the “innocuous-sounding” act as part of the right’s war on birth control, writing that “the sneakiness can reach the point of absurdity.” Last week, it became clear that she was right. Independent journalist Rachel Wells broke the story of an unnamed Tennessee woman who explained during a town hall meeting in Jonesborough that she had been denied prenatal care because she was unmarried—a condition that apparently went against her provider’s “Christian values.” (In case you were wondering, marital status is not a protected class under federal civil rights law.) She is now traveling out of state to receive care and has filed complaints with the Department of Commerce and Insurance and the American Medical Association. According to Wells, this is the first reported case (at least in recent history) of an American woman being denied prenatal care for being unmarried. But the funny thing—and yes, there’s always a funny thing—is that some of the most important theological figures were born out of wedlock. Ishmael was the son of Abraham and his servant Hagar. Mary became pregnant with Jesus before she was married to Joseph. Cain and Abel? Their parents couldn’t be married because the concept didn’t even exist in the first half of Genesis. What has always existed within Christian ideology is kindness and the love of Christ to all, even those you disagree with, just like it says in those He Gets Us commercials (which, again, is something the Christian right doesn’t even follow). Maybe the Tennessee legislature missed that day of Sunday school. Or perhaps this has nothing to do with faith and everything to do with laying the groundwork for the white, Judeo-Christian, heterosexual nation of JD Vance’s wet dreams. My money’s on the latter. AND:
 WARNER AND HIS INCREDIBLE SMILE AT A TELEVISION FESTIVAL A FEW YEARS AGO. (VIA GETTY IMAGES)
 FOLLOW THE METEOR Thank you for reading The Meteor! Got this from a friend? |

Trump's Updated EMTALA Guidance Tells Docs, "You're On Your Own"
BY SHANNON MELERO AND NONA WILLIS ARONOWITZ
On Tuesday, the Trump administration rescinded guidance the Biden administration had issued in 2022 explicitly stating that hospitals are to provide abortion care to patients in emergency medical situations, even if the hospital is located in a state with an abortion ban. The guidance came just as news of desperately ill pregnant women being turned away from hospitals was beginning to emerge, and it clarified the Emergency Medical Treatment and Active Labor Act (EMTALA), a 1986 law that requires hospitals receiving federal funding to provide stabilizing care for any individual experiencing a medical emergency. This week, the Center for Medicare and Medicaid Services said in a statement that the 2022 guidance did “not reflect the policy of this administration” and that it would “work to rectify any perceived legal confusion and instability created by the former administration’s actions.”
Which is ironic, because the thing currently creating massive confusion among providers, patients, and the media is the rescission of the guidance, not the guidance itself. Allow us to clarify: EMTALA has not been repealed; it is still the law of the land and, should you need care in an emergency, your nearest hospital is obligated to provide it or to transfer you to a facility that can—yes, even if that care includes an abortion.
“I want patients to know that nobody should be denying you care because of this memo,” Dr. Dara Kass, a former regional director at the Department of Health and Human Services and an emergency physician in New York, tells The Meteor. And if you do think your providers violated EMTALA, she notes, you can still issue a complaint.
So what’s the purpose of the memo, if it doesn’t change the law? Trump may just be looking for a way to pay lip service to the anti-abortion movement. And the memo’s specific language may also be strategic, as Jessica Valenti points out in her newsletter: The CMS memo says EMTALA still requires treatment of “emergency medical conditions that place the health of a pregnant woman or her unborn child in serious jeopardy.” The phrase “unborn child” (which also appears in EMTALA) hints at fetal personhood and sets up a showdown between a woman who has a life-threatening condition, like an ectopic pregnancy, and her fetus.
It’s all very chaotic. And chaos is the point.
“This action doesn’t change hospitals' legal obligations,” Fatima Goss Graves, president of the National Women’s Law Center, said in a statement, “but it does add to the fear, confusion, and dangerous delays patients and providers have faced since the fall of Roe v. Wade.” Dr. Kass adds that while the 2022 guidance “signaled to doctors that the government had their back,” the rescission tells doctors, “You’re on your own” and erodes their confidence that the government will protect them. There will inevitably be more “physicians who are not sure what they’re allowed to do,” she says, “and therefore they might do less.”
Meanwhile, more pregnant patients will suffer as doctors are forced to contend with legal quandaries under pressure. We’ve already seen what happens when emergency rooms are slow to act; Amanda Zurowski, Kaitlyn Joshua, and Amber Nicole Thurman have each paid the price for a hospital’s confusion over what doctors are allowed to do—Thurman with her life.

For better or worse, Dr. Kass doesn’t see this latest move as dramatically changing “the care on the ground.” (Indeed, even with the 2022 guidance in place, there have been dozens of documented cases of pregnant women being denied emergency care or treated negligently.) Rather, she sees this as “a distraction from what we need to do—which is to reinstate access to abortion services in every state.”

New Abortion Chaos in the ER
  June 5, 2025 Greetings, Meteor readers, My two loves, Aryna Sabalenka and Coco Gauff, will be facing off at the French Open this weekend. While I cannot decide who to root for, Gauff taking the trophy would be historic, as an American has not won the French Open in a decade. I’m willing to be pro-America this one time.  In today’s newsletter, we try to wrap our heads around the Trump administration’s latest anti-abortion move. Plus, your weekend reading. Bonne nuit, Shannon Melero  WHAT'S GOING ONThe chaos is the point: On Tuesday, the Trump administration rescinded guidance the Biden administration had issued in 2022 explicitly stating that hospitals are to provide abortion care to patients in emergency medical situations, even if the hospital is located in a state with an abortion ban. The guidance came just as news of desperately ill pregnant women being turned away from hospitals was beginning to emerge, and it clarified the Emergency Medical Treatment and Active Labor Act (EMTALA), a 1986 law that requires hospitals receiving federal funding to provide stabilizing care for any individual experiencing a medical emergency. This week, the Center for Medicare and Medicaid Services said in a statement that the 2022 guidance did “not reflect the policy of this administration” and that it would “work to rectify any perceived legal confusion and instability created by the former administration’s actions.” Which is ironic, because the thing currently creating massive confusion among providers, patients, and the media is the rescission of the guidance, not the guidance itself. Allow us to clarify: EMTALA has not been repealed; it is still the law of the land and, should you need care in an emergency, your nearest hospital is obligated to provide it or to transfer you to a facility that can—yes, even if that care includes an abortion. “I want patients to know that nobody should be denying you care because of this memo,” Dr. Dara Kass, a former regional director at the Department of Health and Human Services and an emergency physician in New York, tells The Meteor. And if you do think your providers violated EMTALA, she notes, you can still issue a complaint. So what’s the purpose of the memo, if it doesn’t change the law? Trump may just be looking for a way to pay lip service to the anti-abortion movement. And the memo’s specific language may also be strategic, as Jessica Valenti points out in her newsletter: The CMS memo says EMTALA still requires treatment of “emergency medical conditions that place the health of a pregnant woman or her unborn child in serious jeopardy.” The phrase “unborn child” (which also appears in EMTALA) hints at fetal personhood and sets up a showdown between a woman who has a life-threatening condition, like an ectopic pregnancy, and her fetus. It’s all very chaotic. And chaos is the point. “This action doesn’t change hospitals' legal obligations,” Fatima Goss Graves, president of the National Women’s Law Center, said in a statement, “but it does add to the fear, confusion, and dangerous delays patients and providers have faced since the fall of Roe v. Wade.” Dr. Kass adds that while the 2022 guidance “signaled to doctors that the government had their back,” the rescission tells doctors, “You’re on your own” and erodes their confidence that the government will protect them. There will inevitably be more “physicians who are not sure what they’re allowed to do,” she says, “and therefore they might do less.” Meanwhile, more pregnant patients will suffer as doctors are forced to contend with legal quandaries under pressure. We’ve already seen what happens when emergency rooms are slow to act; Amanda Zurowski, Kaitlyn Joshua, and Amber Nicole Thurman have each paid the price for a hospital’s confusion over what doctors are allowed to do—Thurman with her life. For better or worse, Dr. Kass doesn’t see this latest move as dramatically changing “the care on the ground.” (Indeed, even with the 2022 guidance in place, there have been dozens of documented cases of pregnant women being denied emergency care or treated negligently.) Rather, she sees this as “a distraction from what we need to do—which is to reinstate access to abortion services in every state.” —Shannon Melero and Nona Willis Aronowitz AND:
 IT'S BACONEGGANDCHEESE YOU CRETIN.
 WEEKEND READING 📚On mothers and daughters: Molly Jong-Fast unflinchingly traces the mental decline of her mother, iconic feminist novelist Erica Jong, in this excerpt from Jong-Fast’s memoir How to Lose Your Mother, which came out last week. (Vanity Fair) On always being here: It’s time to learn about the key trans figures in history that get cut out from school lessons. (Erin Reed in the Morning) On Dyke Day: How a beloved Pride tradition stays alive without being beholden to flipflopping corporate sponsors. (LA Public Press) On beauty: Meteor collective member Raquel Willis reminds us that, against all odds, trans people are here to stay and will still be “seen in all of our glory.” (Atmos)  FOLLOW THE METEOR Thank you for reading The Meteor! Got this from a friend? |

Is the Last Abortion Haven in the Caribbean Closing?
How U.S. influence has been quietly reshaping access in Puerto Rico
By Susanne Ramirez de Arellano
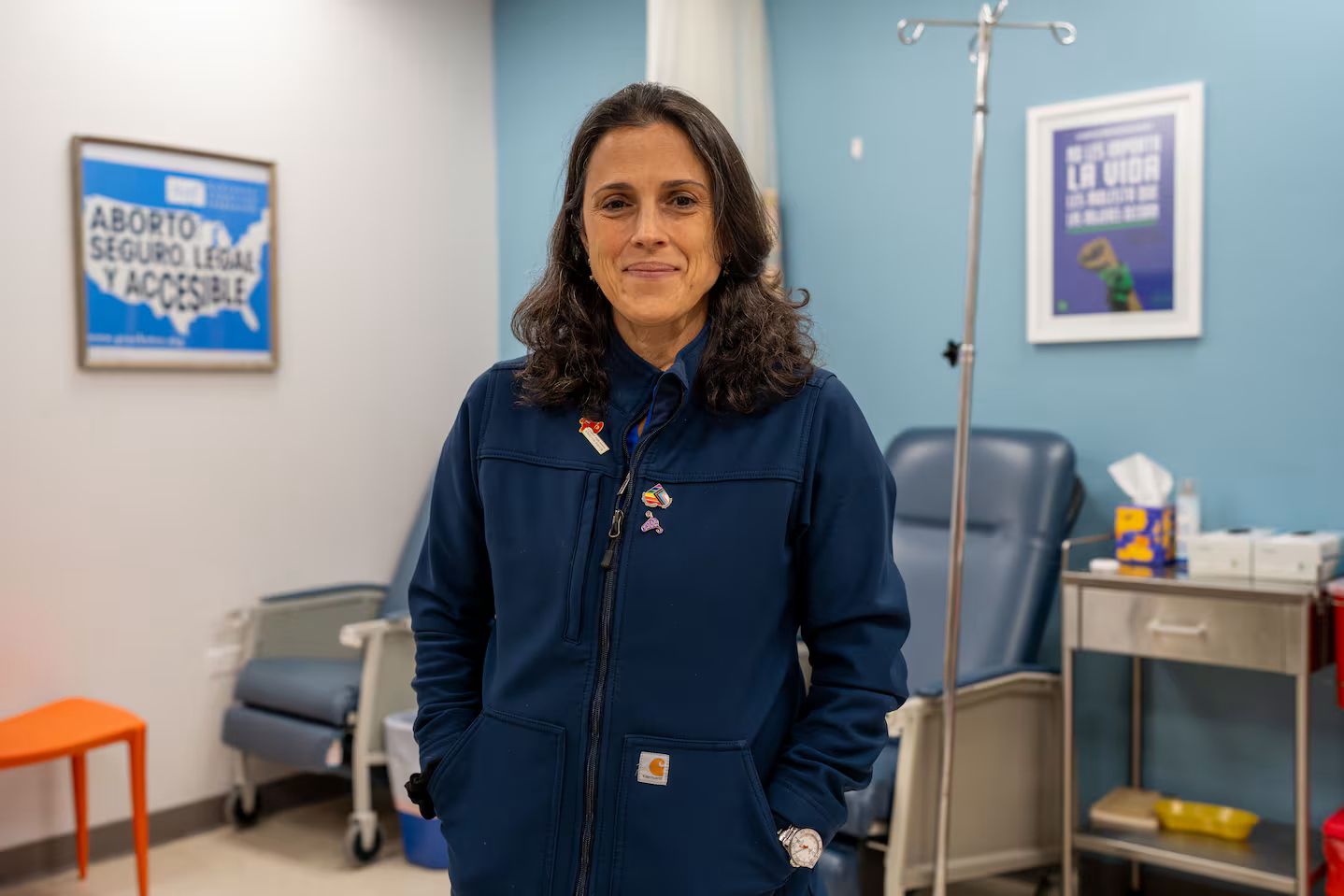
Dr. Yari Vale's petite frame is no longer weighed down by the nine-pound bulletproof vest she wore when anti-abortion threats increased after the end of Roe v. Wade, but she hasn't gotten rid of it. The security guard at Dr. Vale's Darlington Medical Associates clinic in Río Piedras is no longer at the door; still, she has him on standby. With the return of Donald Trump to the White House and Jenniffer González, a Trump devotee, in the governor’s seat, Dr. Vale is bracing for an escalation in the fight to safeguard reproductive rights in Puerto Rico.
The predominantly Catholic island is “on paper one of the most accessible places in the Western Hemisphere” to obtain an abortion, NPR reported just after Roe was overturned. But with the U.S.'s shift toward right-wing Christian nationalism, that could be changing.
Dr. Vale, an OB/GYN at the Darlington clinic—the only one of the island's four that does late-term abortions—is on the frontline of the fight to keep what’s happening in the United States from happening in Puerto Rico, euphemistically called an unincorporated territory (it's a colony, really). It's a battle that, she says, feels like “throwing a firecracker up in the air, and it's just smoke and no one hears you.” But she persists, knowing that the first line of defense is the clinics.
The Legacy of Pueblo v. Duarte
For years, Puerto Rico has been known for its liberal abortion laws: The right is enshrined in the island’s constitution (which exists separately from the U.S. Constitution) and is protected by the right to intimacy under Puerto Rico’s penal code. Abortion is legal on request if it is performed (or prescribed) by a physician to protect the pregnant woman’s life or health—and health includes mental health. There are no limits (abortion may not be banned before viability; post-viability abortions are permitted for the preservation of the pregnant person), and the procedure doesn't require the consent of partners, ex-partners, or, in the case of minors, parents.
However, these laws have their roots in a dark colonial history. In 1902, four years after invading the island, the U.S. enacted policies to control the population, although abortion was still prohibited without exception. Then, in 1937, colonialists who wanted to further limit the Puerto Rican population passed legislation based on racist neo-Malthusian and eugenic theories, virtually legalizing abortion on the island if it was to protect the life and health of the patient. These changes later facilitated clinical trials of the contraceptive pill and mass coerced sterilizations—a procedure that became so common that it was known among Puerto Rican women as “la operacion.”
In 1980, a case involving a minor and her doctor went even further, and set up modern abortion law in Puerto Rico. In the landmark Pueblo v. Duarte, Dr. Pablo Duarte Mendoza, who had performed an abortion on a 16-year-old girl in her first trimester, was sentenced to four years in prison. He appealed, and the Puerto Rican Supreme Court agreed with him, stating that through the island’s penal code, abortion is legal if it is performed to save the woman's life or health, including mental well-being.
Like many things on an island impacted by colonialism, abortion access is still limited for everyday Puerto Ricans. A surgical abortion costs $250, and a medication abortion between $300 and $350; meanwhile, about 43% of Puerto Ricans live below the poverty line, and insurance plans on the island do not cover abortion. And in addition to cost, religion and social stigma—the “what-will-my-family-say” factor—serve as deterrents for many women.
The Dobbs Effect
When 2022’s Dobbs v. Jackson Women’s Health Organization decision removed the constitutional right to an abortion in the U.S., it didn’t automatically affect rights in Puerto Rico (unlike on the mainland, where “trigger bans” were in place). In fact, some U.S. women began to travel to Puerto Rico from states with restrictive abortion laws, such as Florida. It was the return of the “San Juan holiday.”

But Dobbs did embolden conservative Puerto Rican politicians and pro-life groups, who saw a window of opportunity and seized it. Shortly after the decision, the right-wing religious party Proyecto Dignidad (PD) adopted the U.S. anti-abortion lobby's blueprint and tried to push through several bills to curtail access to abortion, and even criminalize it. They argued that the end of Roe implicitly negated Pueblo v. Duarte. The Senate ultimately defeated the bills; according to many Puerto Rican legal experts, Pueblo v. Duarte rests on the Puerto Rican penal code, which has no analogy in the U.S. Constitution—and should, therefore, not be affected by Dobbs.
An Ascendant Right-Wing Movement
Abortion-rights advocates warn that efforts to criminalize abortion in Puerto Rico are not over. Traditionally, “the issue of abortion in Puerto Rico has not been the overriding controversy that the anti-abortion and ultra-religious politicians want to make it out to be now,” says Senator Maria de Lourdes Santiago, a lawyer and Senator for the Puerto Rican Independence Party (PIP). But, she says, the anti-abortion campaign orchestrated by Proyecto Dignidad now "magnifies the issue to demonize it."
Founded in 2019, PD has capitalized on its nexus of Catholic and Evangelical churches; the erosion of the traditional duopoly of the pro-statehood New Progressive Party (PNP) and the Popular Democratic Party (PPD); and an increasingly ultra-conservative sector of the population urging a return to traditional values. Even though the party got only seven percent of the vote in the 2024 elections, its influence is strong island-wide, with a campaign that now hinges on the abortion issue.
Proyecto Dignidad Senator Joan Rodriguez Veve, a canon lawyer and face of the populist religious right, has vowed to continue fighting to restrict access to abortion. She recently introduced legislation, PS 297, restricting access to abortion for adolescents under the age of 15. The bill is a carbon copy of one that the Puerto Rican House rejected a year ago. It calls for jail time for any doctor or person who assists a minor in getting an abortion, and a slew of other measures, including forensic interviews of minors seeking an abortion.
The Senate approved the bill in February, and almost everyone I spoke to—politicians, legal experts, and abortion doctors—told me they believe it will pass, even though both pro-abortion and some anti-abortion groups have, for different reasons, voiced their opposition to the measure.
A New Generation Stands Up

At the same time that PD is gaining influence, attitudes about abortion are shifting with the younger generation. Rising numbers of people support abortion rights, and young people have galvanized around the issue, taking to the streets in protest and amplifying groups like Aborto Libre Puerto Rico, Profamilias, and Proyecto Matria, among others. It’s a generation that, unlike its mainland counterpart, grew up without a sense of abortion as a wedge issue.
Most recently, health professionals and activists have spoken out against PS 297, warning that the bill puts women and girls in danger. “What's going to happen here is that young women and those most vulnerable will seek out illegal abortions and go to the places where illegal drugs are sold to purchase abortion pills, many cut with fentanyl, in doses that are not recommended,” says Puerto Rican feminist activist Alondra Hernández Quiñones.
As religious and conservative groups gain traction in Puerto Rico, Dr. Vale worries that a girl of 15, whose parents are ultra-conservative and refuse to consent to her abortion (as the new legislation would require), would be forced into motherhood. Clinics like Darlington have stopped seeing patients younger than 15 at all, and Dr. Vale fears a future where abortion, currently a safe and regulated procedure, “will once again be a public health problem…where we don't know how many women end up in emergency rooms due to an [unregulated] abortion gone wrong.”
“This worries me a lot,” says Isharedmie Vazquez, a 17-year-old Puerto Rican student. “It seems incredibly wild to me that instead of guaranteeing secure options [for an abortion], what they are looking for is to criminalize it and force women to assume a responsibility for which they are not prepared. It's unfair that they want to take away the right to decide about our lives.”
 Susanne Ramírez de Arellano is an author on race and diversity, opinion writer, and cultural critic. The former news director of Univision, she writes for NBC News Think, Latino Rebels, and Nuestros Stories, among other outlets.
Susanne Ramírez de Arellano is an author on race and diversity, opinion writer, and cultural critic. The former news director of Univision, she writes for NBC News Think, Latino Rebels, and Nuestros Stories, among other outlets.