
Let's Take This Outside
The never-ending work to diversify the great outdoors
By Shannon Melero
Rockland State Park, nestled in Upper Nyack, New York, was a summertime staple of my youth. Every year, my family would pile into a car with coolers, chairs, bags of charcoal, and enough groceries to feed a small army and make the hourlong sojourn from the Bronx first thing in the morning to secure a spot on the grass. Location was everything. We needed a flat surface to set up games and blankets, but also had to be close to one of the grills the park provided, and most importantly, we needed to be a reasonable walking distance from the park’s massive pool.
I didn’t realize it at the time, but those trips to Rockland were my first introduction to the great outdoors, a relationship which years later would blossom into a love of hiking and staring at trees.

What made Rockland such a comfort was that everywhere I looked, I saw families that mirrored my own. Huge groups of Latine and Black people gathered around decaying wooden picnic tables, laying out tubs of familiar foods our matriarchs had cooked the night before—potato salads; three different preparations of rice; pork; and pasteles, all of which would be handed out at dinnertime. Rockland was a full-day experience from sunup to dusk.
But like many outdoor locales that attracted urbanites of color, Rockland State Park was segregated up until the late 1950s, so the fact that I saw so many families of color in one area wasn’t mere happenstance. It was, historically speaking, where we had been gathering all along.
The idea of “public lands” goes back as far as the 1780s, when states began ceding land rights to the newly formed federal government. Since that time, the idea of who gets to be outside, where, and when has been racially inflected. While the restrictions have now changed—anyone can travel or pay a fee and go to any national or state park—their impact lingers. In 2025, outdoor publication The Trek found that 96% of long-distance hikers on the Appalachian Trail were white. Meanwhile, the Trump administration has enacted its own efforts to make the outdoors white again.
“I always say that white people were really onto something when they invented the great outdoors and then gatekept it,” Chevon Linear, co-founder of Black People Outside, tells me. Chevon, who goes by Chevy, is warm and inviting, even through the computer screen that separates us. Chevy was a Girl Scout as a child but notes that, “The outdoors were really deemed as ‘white people shit.’” It’s a common term we use when referring to the outdoors, and while it’s often said in a joking manner, it’s a genuine phenomenon. For much of American history, going outside for leisure was a privilege—a prohibitively expensive one that has now become a trillion-dollar industry by catering mostly to white, affluent outdoor enthusiasts.

Chevy founded Black People Outside with her fiancé, Kameron Stanton, after an impromptu trip to Grand Teton, a national park in Wyoming, six years ago. The couple, who had never camped before, traveled with one of Chevy’s friends, who loaned them all of the gear they needed. Kameron called the experience “spectacular.”
“The true dark night sky, the energy from everyone around you…everyone was just so nice,” he recalls. “And it's like, dang, outdoors got everyone acting friendly.”
For Chevy, who had traveled all over the world before the pandemic, that night in Grand Teton sparked a calling. “Just seeing the stars, I was crying,” she recalls. “I had never seen the sky like that. It was truly quiet and I’d never heard it so quiet before.” But what she didn’t see were many other Black people. “I’m from Chicago, so I’m used to seeing Black people everywhere I turn,” she says. Witnessing the beauty of nature and the profound silence that brought her peace. She knew she had to share the experience with more people.
“I just feel like we have these irrational fears about the outdoors because of our past,” Chevy says. “As Black people, we were outside because we were escaping, running through the woods for survival. It wasn’t for joy.”
As Chevy and Kameron embarked on their mission, forming what would eventually become Black People Outside, they came across the same barriers that many communities of color face: limited access to green spaces, high costs, and that age-old idea that going outside was just more white people shit. Then, as with so many things, there’s the barrier of representation. In 2018, a writer at the University of Toronto described advertising around the outdoors as “visual apartheid.” Chevy, at least, had the Girl Scouts when she was young, but Kameron says he had no sense of Black people in the outdoors at all until he reached adulthood. “I remember growing up watching TV, the only people that was on there hiking and being outside and skiing…was white people and Dora [the Explorer],” he says. “She was in the streets with the backpack, and I was there with her. But the reality is Black people [not seeing themselves represented] contributes to the disconnect that we sometimes have with nature.”
Chevy and Kameron refer to all of these as invisible barriers, most of which they’ve been able to overcome through educational programming, community outreach, and working with brands to provide gear to those without. But one additional extremely visible barrier has many outdoors people reconsidering their plans for the summer: the Trump administration.
In his second term, Trump rolled out massive budget cuts to the National Park Service, changed admission costs for non-U.S. citizens, and relaxed hunting regulations, which puts both forest animals and backcountry hikers in more danger. Then there are the non-park-related factors that have made it more difficult than usual to just go outside as a person of color—ICE, emboldened white supremacists, and most recently, gas prices. Outside isn’t just reverting to white people shit; it’s turning into wealthy white people shit.
The founders of Black People Outside, though, refuse to flinch.

“I’m gonna do what I wanna do and go where I wanna go, and I want our people to have that same energy,” Linear says. “National parks are not the only place to recreate. We still have state parks, we have county parks. We are going to be outside.” For Linear, it’s not a euphemism or a business slogan; it’s a fact. She will not be pushed back indoors, and she is adamant that no other outdoorsperson feels alone or unsafe.
Although Chevy, Kameron, and I are speaking with each other for an interview and are complete strangers, our mutual love of the outdoors creates a level of comfort. I share with them stories of hiking with my daughter. We laugh about the time I misread a map and had to scramble down an enormous rock with a one-year-old on my back and my mother —who vows she will never do that trail with me again—yelling at me for dragging her out to the wilderness. I relay my fears and discomfort over what this summer may hold as I try to go outside with my daughter, to create the same kinds of core memories my mother made for me all those years ago at Rockland State Park, before I ever had to wonder if the hiker next to me questioned if I belonged on a trail.
“You have to attack ignorance with your presence,” Kameron says. “Ain’t nothing going to change if you end up hiding.”

Did Trump Ruin the Workplace?
 May 29, 2026 Did Trump Ruin the Workplace?Three women reflect on the evolution of misogynyBY MARIN COGAN Earlier this year, 2016 nostalgia took over social media, with our friends posting wistfully about their more naive selves. The trend quickly ran its course, but that decade, from 2016 to 2026, has seen huge change—for politics, culture, the world. And it made us wonder: What’s different from then to now, particularly when it comes to women’s lives? What have we lost, and maybe gained? We'll be exploring this topic this summer, and we're starting here, with a deep dive on how work and the professional sphere have changed—or not—for women. A lot can happen in a decade. Around this time ten years ago, Americans were still debating whether to take the new Republican presidential nominee, Donald Trump, seriously. Global pandemics seemed like old-timey problems; artificial intelligence was still mostly in the realm of science fiction. The culture back then was different, too. In various industries, women were starting to speak out about workplace harassment and abuse. Others made noise about the chronic lack of representation of women and minorities. The discussions pressed both big companies and individual actors to acknowledge wrongdoing and work towards more just and equitable workplaces. And then came the backlash: the comebacks, the anti-woke movement, the defamation lawsuits, the assault accusations ignored, the startling rise of the manosphere. Ten years later, we are living in the aftershocks of that era, both the progress made and the retaliation it inspired. The Meteor spoke with three women–leaders in government, tech, and Hollywood–about what’s changed in their workplaces for women in the last decade, for better and for worse.  CLAIRE TRICKLER-MCNULTY IN 2022, WHEN SHE CAME TO GENEVA TO PRESENT AT THE COMMITTEE ON THE ELIMINATION OF RACIAL DISCRIMINATION. (COURTESY OF CLAIRE TRICKLER-MCNULTY) Used to ICE’s Old Boys’ Club, She Became the Target of a Sexist AttackClaire Trickler-McNulty, a lawyer, served as a Deputy Assistant Director at Immigration and Customs Enforcement (ICE) under Obama and during Trump’s first term, then as an Assistant Director there during the Biden administration. She witnessed dramatic swings in rhetoric and policy between administrations, and ultimately became the target of a deeply partisan investigation by House Republicans, who accused her of trying to push a “woke agenda” inside the agency—claims she says were baseless. Trickler-McNulty is now a policy fellow at Hyphen and co-hosts a podcast called The Melting Pod about immigration. There were some efforts under Obama, and then under Biden, to encourage the hiring of more female officers. But the whole time I was there, law enforcement was still predominantly male. If I hadn’t been a lawyer, I would never have been in those rooms. There were definitely parts of ICE that felt like old boys’ clubs—cliques of men where you had no hope of getting into their inner circle of leadership. When I took maternity leave the second time in 2015, my boss told me…that the real burden of maternity leave is on men, because they have to pick up for women who are taking leave. Which is not what you want to hear from your boss as you're taking maternity leave. I befriended a lot of female law enforcement officers during my time there. I wanted to support women moving into leadership positions because I knew it was a gendered environment. I saw a number of women–really good, dedicated law enforcement officers–repeatedly passed over for promotions in favor of men. The women would tell me, “The guys who get promoted are the ones who go drinking with the boys, who go to strip clubs together.” I absolutely saw women get passed over while less qualified men moved up through these networks. That was happening during the Biden administration. It’s recent history. [But] under the first Trump administration, things changed significantly…It definitely felt like more men were being elevated into leadership positions. A certain clique became more ascendant. That said, the [changes of the] first Trump administration felt slower to me. It was more like watching sandcastles slowly get washed away. That’s part of why I wanted to go back into government later. There was still so much detention reform work to do, like trying to implement the Prison Rape Elimination Act. I felt like so much of what we had tried to fix had been washed away, and I still had this fire in me to try to fix some of it. And then, in 2023, I got heavily attacked by the far right. Part of it absolutely felt gendered. I think I was an easier target because I was a woman on the West Coast with a hyphenated last name. When I look at younger women coming up now, I do see progress in how they interact with men and set boundaries. That makes me happy. But then I look at what’s happening at the senior levels, and it doesn’t feel like there’s been nearly as much progress there. I still think about the moments where…women reported harassment and leadership just shrugged. Those are the things I feel guilty about, especially because I was a supervisor. Looking back, I wish I had been less afraid. Less worried about making men angry. Less worried about what they thought about me. More secure in myself and in what I was doing.  TRACY CHOU AT WORK. (COURTESY OF TRACY CHOU) She’s a Tech Worker Who Started at Google—and Became an Anti-Harassment AdvocateTracy Chou started her tech career with internships at Google and Facebook before becoming a software engineer at Quora and Pinterest. In 2013, Chou posted a viral Medium post about the lack of publicly available data about women in engineering roles at tech companies. Chou earned media recognition and awards–but also backlash from male colleagues and internet trolls. Later, she founded Block Party, a digital anti-harassment tool. Quora was this new question-and-answer platform when I was there in 2010-2011, and we needed content for the site. So all of us who worked there were trying to generate content. I found my little niche answering questions about being a woman in engineering. I had colleagues who really didn't like it and would act out. Sometimes they would try to undermine me, or complain about me [advocating for representation of women.] I had one Asian engineer say to me, “Engineering is the one thing that Asian guys have. Why can't you just let us have it?” And other people who complained to me about how we already lowered the bar so much for women and minorities, do we have to lower it even more? I felt like I had to overperform as an engineer. I remember getting in super early to the office, working really late, and trying to create that extra space for diversity work on the weekends, so that it wouldn't feel like it was taking away from my main job. Probably around 2018, my platform had gotten a bit bigger. I started experiencing more pile-ons, but there was still also targeted harassment from individual people who would go pretty deep–I had instances with thousands of trolls on Reddit, and then some of that spilled over onto 4chan, and those people started coming after me too. Then I also had to deal with people who became obsessed with me. There was one guy who was stalking me. He lived internationally but showed up in San Francisco multiple times. Block Party came directly from the experience of dealing with harassment myself and from having seen it on platforms I had previously helped build. I was frustrated by companies saying, “Abuse and harassment are really hard problems to solve.” I thought: It’s not that hard. I’m sure you can do better than what you’re doing now. I had literally worked on some of these platforms [so I knew it was possible]. And I had also been the target of abuse and harassment myself. The silver lining is that I was able to take that firsthand experience and turn it into better solutions—not just for myself, but hopefully for other people too. All the diversity efforts and the MeToo movement impacted the tech industry in similar ways. If you look at computer science enrollment numbers, many more girls are enrolling and graduating with computer science degrees. There are also many more female founders now. The whole ecosystem seems to have improved, and there are many more efforts supporting women in tech, women in VC, women in engineering, and underrepresented minorities more broadly. I also think the general cultural awareness around these issues has increased dramatically. Ten or 15 years ago, most people didn’t know what intersectionality meant. Now, many people are at least familiar with the concept. That’s all positive. What’s worse is the recent backlash and demonization of DEI—the fact that people feel so emboldened to be loudly and proudly anti-DEI. I expected progress to be slow. I didn’t expect this level of aggressive backlash. Still, the work will continue in some way. So overall, I’m still mildly optimistic. But I also feel tired of fighting.  AMY ADRION, RIGHT, ON SET DURING HALF THE PICTURE. (PHOTO BY ASHLY COVINGTON) She’s a Director For Whom “MeToo Absolutely Mattered”Amy Adrion is an Emmy-nominated writer and director. Her 2018 film, “Half the Picture,” examined the experiences with systemic discrimination faced by women directors in Hollywood. She has also directed episodes of Storyline Online, and teaches filmmaking at Rochester Institute of Technology. I never had any particular instance of sexual harassment or overt discrimination. I worked as a production assistant, as an assistant director, and as a low-level crew member on tons of independent films. I worked for a distribution company in New York at the time when [Harvey Weinstein’s] Miramax was the big player in town. I went to Sundance and all the film festivals. I never personally had a negative experience in my early career in film. But I do think the issue was less about individual moments of discrimination and more about the fact that the people in power tended to be white men from a certain cohort, and they responded to the stories that connected with them. And so you would have these breakout films by women directors at festivals [and then] you would see them kind of drop out of the cultural conversation after 10 years. I think that is discrimination in a broader sense. The stories that make women, nonbinary, or gender-expansive people feel better about being themselves just haven’t had as many people in positions of power supporting them. As frustrated as I am by the current state of things, it would be totally disingenuous to say nothing has changed. A lot has changed. You look at the stories that are being made now, and they’re very different from what was in theaters or on television 20 years ago. There is more diversity of voices and stories being told. Is it enough? No. And it’s frustrating because there was this energy around diversity and hiring different voices–especially around 2020–and it definitely feels like there’s been a backslide. A lot of women directors I know who finally got their first TV episode, or maybe their second, aren’t really getting hired anymore because the business is contracting. MeToo absolutely mattered. It was an important movement that had a real impact. Harvey Weinstein is in jail. You can’t say it came and went without consequences. It was necessary and important, and it’s had lasting repercussions. That said, I think MeToo also created a lot of discomfort among people in power, and that discomfort led to backlash. When I started making “Half the Picture,” I interviewed some women who had been part of a group inside the Directors Guild back in the early ’80s who were looking at the numbers of women working as directors and agitating for change. They were probably in their sixties when I interviewed them, and while they were grateful there was renewed attention on discrimination against women directors, they also had this very world-weary attitude of, “Oh, this again.” At the time, I was very much like, “No, this is different. Things are changing. The ACLU is investigating. Women are speaking out. We’re finally making progress.” And now, 10 years later, I find myself with a much more cautious optimism. I think human beings naturally assume things just evolve and get better over time—that progress is inevitable. But it’s not. If the last 10 years have taught us anything…it’s that you have to keep fighting for these rights constantly, or they will be threatened or taken away. That was a hard lesson for me to learn in my forties. The interviews have been edited for clarity and length.  ABOUT MARIN COGANMarin Cogan is an independent journalist. She was most recently a senior correspondent at Vox and has worked as a writer for New York magazine, GQ, ESPN the Magazine, and other publications.  ENJOY MORE OF THE METEOR Thanks for reading the Saturday Send. Got this from a friend? Don’t forget to sign up for The Meteor’s flagship newsletter, sent on Tuesdays and Thursdays. |

The Toni Morrison approach to mothering
Black women deserve to claim and relish the depths of freedom motherhood can bring.
By Rebecca Carroll
When I was nursing my son as a baby, he started doing this thing where he would latch the little fingers of his free hand around my bottom lip, and then proceed to slowly knead at it in a small but persistent effort to pry open my mouth. It almost felt like he was trying to find some sort of entryway back into my body. Once, when he was about two, I softly placed my hand over his as he tugged at my lip, and asked in a whisper, “Does this feel like love to you?” He stared back at me with his beautiful, bright eyes, and nodded “yes.” It felt like love to me, too.
I am reminded of this hushed exchange of heartwork between us whenever I see one of these pieces about “styles of parenting” that crop up online every now and again, introducing or reintroducing terms like “attachment parenting,” “helicopter parenting,” “gentle parenting,” and “intensive parenting.” The methods they describe might sound fresh, but they’re often adjacent to the four Mayo Clinic-approved styles of parenting, which have been around since the 1960s—authoritative, authoritarian, permissive, and uninvolved. And they almost always feel white-coded, not just because labeling (or, let’s be honest, marketing) how parents interact with their children is about having the time and the income to ponder how you might like to categorize your “style” of parenting. These terms also dissociate and intellectualize what is, to me, and to many Black mothers I know, an emotionally freeing, visceral experience.
It is striking to me how little the experience of Black mothers factors into the standard offerings on how to parent today. Instead, we get media portrayals of Black mothers as struggling single moms and “modern-day mammies,” or neck-rolling, meme-friendly, “You got McDonald’s money?” kinds of stereotypes. But Black mothers are, and Black mothering is, so much more than that. And we deserve to claim and relish the depths of freedom mothering can bring——especially given the inherent, deeply harrowing history of when and if we were even able to keep our children.
Morrison offers this piece of advice: “When they walk in the room, my face says I’m glad to see them.”
No one knew that better than the late novelist Toni Morrison, who was herself a single mother of two boys. Becoming a mother, Morrison said in a 1989 conversation with Bill Moyers, “ was the most liberating thing that ever happened to me.” The demands of her children, she went on to explain, were not like those of her colleagues, friends, or lovers. “Somehow all of the baggage that I had accumulated as a person about what was valuable just fell away. I could not only be me—whatever that was—but somebody actually needed me to be that.” That’s exactly how I felt when I was nursing my son, when he needed me to be that person who would feel like love.
Later, years after I stopped nursing, I snuggled him often and regularly, let him sleep in the bed with us at night, and made myself available to him in ways that felt centered and honest. I seldom missed a call. I always allowed myself to be vulnerable even, and especially, when I didn’t have an answer to solve a problem—while also trying like hell to solve the problem. “If you listen to [your children],” said Morrison, in that same conversation with Moyers, “somehow you are able to free yourself from baggage and vanity… and deliver a better self, one that you like. The person that was in me that I liked best was the one my children seemed to want.” Obviously, we have to make choices, set boundaries, and act as moral compasses for our children, but isn’t that part of delivering the version of ourselves that we like best?
REBECCA AND HER SON, KOFI (COURTESY OF REBECCA CARROLL)
My friend Caryn and I raised our sons, who are just eight months apart, as cousin-brothers, and have frequently mused over the past 21 years about the ways in which parenting Black children is not just about “the talk” for our sons, or warnings about the oversexualization of Black girls for our friends with daughters. It’s about mitigating the harshness of their inevitable reality growing up in America, with the softness of our generational instincts.
Morrison’s approach to parenting squarely challenges the meme and media stereotypes (not that she would have paid them much mind), and blatantly disregards white mainstream guides. Black mothering doesn’t need a name or a category; it deserves a kind of reverence. In simpler terms, Morrison offers this one piece of salient advice: “Let your face speak what’s in your heart. When they walk in the room, my face says I’m glad to see them. It’s just as small as that, you see?”
The summer after my son went to college, I was really struggling with him being away. Like, actually grieving. We sat down one evening to talk about it. I told him how hard it was for me to be physically separated from him, almost as if a part of my body was missing. And he said, “Mom, I’m doing what I’m supposed to be doing. And that’s a testament to you and your mothering.” I’d like to think that is in no small part because my face has always said I’m glad to see him when he walks into a room.
More Mother’s Day reading and watching from The Meteor:
A Feminist Love Letter to Baby Formula
It’s Time to Rethink the Empty Nest
My Abortion Story Is Not What You Think
Three Questions For Tracy Clark-Flory About Motherhood and Sisterhood
Syria's Mothers Are Fighting to Rebuild Their Homes
The Women Who Exposed the "Rape Academy"
Three journalists tell the inside story of investigating a dark global network of men assaulting their partners
By Nona Willis Aronowitz
On March 26, CNN published a 16-minute documentary and interactive story about “a global rape academy,” a network of websites and Telegram chat where men trade tips on how to drug and sexually assault their wives and girlfriends. The story has since been viewed and read by millions, first across Europe and then in the U.S., where the story went viral a few weeks later. Behind the exposé were nearly 25 CNN journalists and staff who for seven months dug into this vast and tightknit community. The Meteor spoke with investigative reporters Saskya Vandoorne and Niamh Kennedy, and reporter and producer Kara Fox, about how this extraordinary investigation came together.
Saskya Vandoorne: It all started with Gisèle Pelicot. I'm the CNN Paris bureau chief here, and I was at the trial down in the south of France [in the fall of 2024] where 51 defendants were on trial for raping her. And I remember very vividly her lawyer speaking about Coco, the platform that Dominique Pelicot had used to recruit all these men to rape his sedated wife. The lawyer described Coco as the weapon of the crime. He said Pelicot had gone on there to find like-minded people. So even though Coco had been taken down, I was curious to find out: Are there any other spaces where men speak to one another about crimes they wanted to commit against their wives or partners?
Kara Fox: We had been reporting out the Dominique Pelicot case, and we knew that Coco users were talking about where to go next on a forum. As we knew that these spaces didn’t go away after the trial, we investigated some of them—other websites and a large Telegram group. One site in particular became the focus, also reported on through the amazing work of German journalists Isabel Beer and Isabel Ströh: Motherless.com. Throughout the course of our reporting we also reported on similar cases, like “the German Pelicot” or “the UK Pelicot.”
Niamh Kennedy: [In the “sleep” groups on] Motherless, there were over 20,000 videos, some showing unconscious women and their eyelids being lifted up to show that they've been sedated. There were more graphic videos as well, sometimes showing what appeared to be nonconsensual sex acts being carried out on these sedated women. It was from spending a lot of time on Motherless that I found a link to the private Telegram group [called “Zzz”]. It featured 1,000 men from all around the world who were giving each other tips on how to drug and rape their partners. It was quite tough, to be honest with you…I definitely felt chills a lot of the time seeing what was going on there. It was very hard.
An upside-down world
SV: There were many conversations that were had before we went undercover [to log onto the site and join the Telegram group to speak to participants]: What did we want to achieve? What could we say? Where was the line? We wanted to remain journalists, so our role was just to ask questions. At no point did we want to encourage any of this behavior; of course, we weren't going to share any pictures or videos of our fictitious wives. So it was very much, sit in this space, ask questions, find out what are they doing, how long have they been doing it for. And also, what was their motivation?
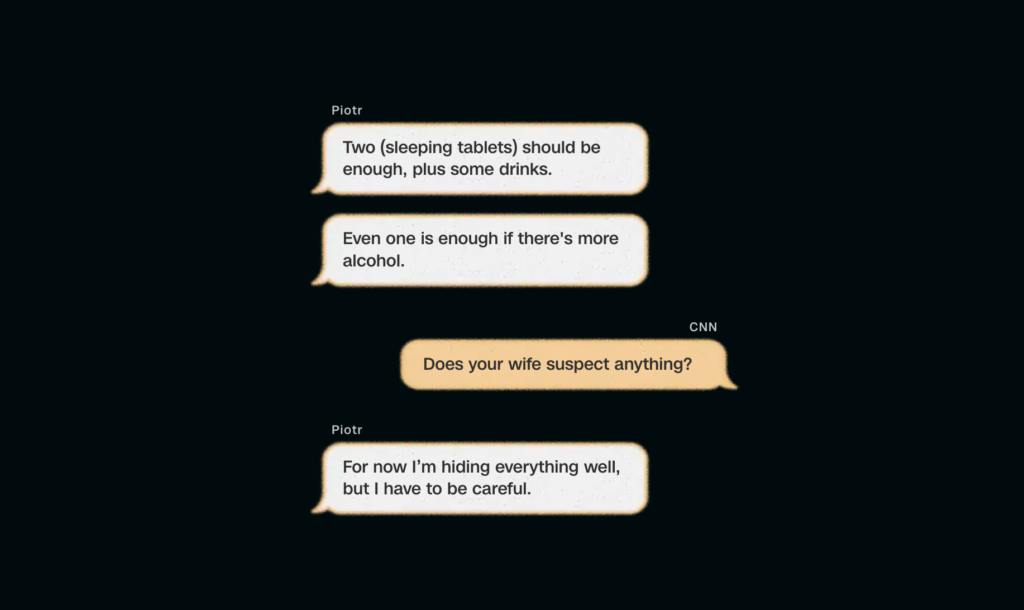
NK: Saskya and I made a shared fake profile, working late into the evening when a lot of the men were online. We spent a lot of time both on the site and in the private Telegram group. There were tiers: men who were selling content, men who were selling sleep liquids—very powerful drugs that could immobilize women. There were men that were offering livestreams. We're talking about hundreds of messages all day long, ping pong, ping pong. They would turn to each other for advice. One guy would write in and be like, "I'm thinking of drugging and raping my wife. Who's done this before?" And one guy would be like, "Yep, I've been doing this for three years. Use this drug." Others would be like, “What weight is she?” “Oh, I did this and I got away with it. " And then a couple of hours later, the man who'd asked the question would post a video and they'd be encouraging each other. It was like a whole brotherhood, where they were really bonding over this shared interest.
SV: [There, the] world is turned upside down. In our world, you've got Gisèle Pelicot, a feminist idol. On Motherless, it's Dominique Pelicot who is the idol. They see him as some kind of god to revere and to emulate.
KF: These users are very comfortable and callous and boisterous. They're not afraid to say what they're doing. They appear to be living in this place where they think they're immune. The psychologist that evaluated half of the men in the [Pelicot] trial told us that they feed on this collective energy of not just the excitement around the abuse, but also allowing themselves to normalize it.
SV: [In the groups] there's this feeling that your wife, your girlfriend, is yours. She is your object to possess, and therefore, it's not rape because you know her, because you're having sex with her anyway. I remember one man said, "Well, I'm not cheating on her. I'm still having sex with her, so she should feel lucky.”
Another way of understanding their mindset is a pendulum swing: Is it because of the emancipation of women, that women are now independent and they have power? Do these men feel under threat? Do they feel like this is a way of getting back the control of being once again the dominant alpha male? Because there is nothing more dominant than a man performing sex acts on an inanimate woman's body. I felt that was fueling some of this behavior.
“A complete shot in the dark”
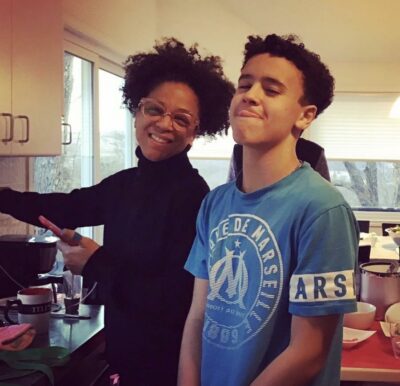
SV: A lot of the men we met in the Telegram group would get very suspicious [of our questions] and the conversations would go cold. But there was this one Polish man, whom we call Piotr in the piece, who was willing to talk and was happy with me being a sounding board, just listening to him and asking questions. I think he was lonely and just really needed to talk. He assumed that I was someone who shared the same fantasies as him, and he was incredibly trusting. And so he would talk about what he was up to that weekend, the holidays he'd go on with his wife and the social activities he would do with his friends. It wasn't all darkness.
One day, Piotr let it slip that he was going to a party at a restaurant.
NK: The thing that made this experience feel more real was when we traveled to Poland to track down Piotr [to confirm that he was real]. He didn’t give us the name of the restaurant, and there was no guarantee that we would find the right place. We were piecing together cryptic clues. We'd figured out based on a photo where he lived, geolocated his house, and then it was just internet research going through all the different restaurants in the area. We found one that had an event which matched the criteria that he'd mentioned. It was a complete shot in the dark.
SV: I remember the party was meant to start at 7:00 and everyone had arrived by 7:05. [Piotr and his wife] still weren't there. I sent a message to Niamh who was standing across the road: "This is the wrong place. They're not going to be here tonight." And then they came out of the car.
NK: When we saw him face-to-face, my heart sank because it's almost like I didn't want it to be true. But everything matched up: the facial identities, the people. He hadn’t been lying.
SV: What was even worse than seeing him was seeing her. Because I'd seen many photos and videos of her. You are a journalist, you're not there to interfere, but I remain a woman. So of course you can't help but think if the shoe was on the other foot, if I were her and she were me, would I want [a journalist] to come and tell me right there and then? And so it was really chilling, unnerving. It was almost a kind of out-of-body experience. I felt like I was watching the scene from up above, and I had to slightly dissociate from my emotions to be able to continue working as a journalist.
Seeing them on the dance floor was also a pretty harrowing moment: She would be dancing with her friends, he would come to join her, and she would leave and sit back down. You just felt that she was kind of fleeing him. Her face had such a vacant expression. This is me projecting, but it was almost as if her body knew what he was doing to it. It was a very strange and cold dynamic.
NK: We're not police officers, but in this case, we felt that we had to do a little bit more [than just observe]. Saskya and I made the call not to approach them because we were very mindful of this woman and her safety, but we did hand our findings in to the police. They were incredibly responsive. [On April 9, Polish authorities confirmed that] they arrested him and he's admitted to all the charges.
SV: We knew the Piotr meeting would be the final stage of the investigation because as soon as we had confirmed who he was, we weren't going to sit on that. So before we got to that stage, we had made sure that we had checked out all the other survivors’ stories that we were going to weave in.
NK: The thing that really brought it all to life was meeting women who, though they weren't directly connected with this group, were survivors of this kind of abuse. The men in this group felt very invisible; they had these shadowy personas. And then when we met people that had been impacted by this kind of harm, that…made it all feel so real. Although I was in awe of their bravery, I was also deeply, in my soul, devastated to see the impact of this.

“A question of whack-a-mole”
KF: The arrival of publication day was a collective exhale. There's been a viral outpouring from survivors; they're flooding our inboxes with stories. Even for us, who know that this sort of abuse has been going on, to see so many survivors coming from the U.S., Australia, Europe, the UK is a lot. And we've seen people talking about their own rape stories and naming their rapists—not necessarily rape that had to do with [drug-facilitated sexual assault], but they felt like this was a moment to reclaim their own narratives.
SV: People began to understand that Dominique Pelicot is not an outlier. He's not unique. This is a phenomenon, and that's why we need to take note of it. The algorithms need greater scrutiny: Some of these guys may be going onto a porn site just watching regular porn, but then they find this slightly darker corner of this website where they're like, "Oh, what is ‘sleep porn’? This is interesting. This is forbidden. Maybe I'll try it out." It is out there, it's not on the dark web, it's easily accessible.
KF: [From a legal standpoint] it looks like there's momentum. In Europe, for example, there's legislation that's being proposed about non-consensual sex and how to define it from a yes-means-yes perspective instead of what exists right now. Several members of the European parliament raised our investigation as proof that more needed to be done. [A majority of the European Parliament approved the “only yes means yes” rape definition on April 28, in order to close any existing loopholes in rape legislation. Irish MEP Maria Walsh said that CNN’s investigation accelerated the debate.]
SV: [We need] more awareness of red flags. We need to ensure that the next time a woman goes to see her doctor and starts complaining about fuzziness or not remembering things she did last week, that if her husband is sitting next to her, the doctor might say, "Hey, can I have a moment alone with you?” So many of these women would go into the doctor's office with their husband, who would then manipulate the conversation like, "Hey, you've been under a lot of pressure, a lot of stress." And police need to recognize that drug-facilitated abuse [happens with] couples in marriages.

Of course, there needs to be better moderation and regulation. In the wake of our investigation, there has been a public outcry here [in France] about Cocoland, [a new site] which has the same interface and is modeled completely on Coco. Just today, prosecutors opened an investigation into this website. But even though the Coco founder has been charged, he's not in custody, and the trial is not set to take place for another year or two. Even today, if you were to go on Motherless, you would still be able to find sleep-content videos on there. So yes, better moderation, but also maybe harsher sentences and real legal repercussions when it comes to these founders. Because let's say tomorrow Motherless is taken down. What's to stop five other websites taking its place? It’s a question of whack-a-mole.
The last thing I’ll say is that if people want these kinds of investigations to see the light of day, you need well-funded news organizations. When [you include] the cameramen, the editors, the people who built the interactive, the lawyers, we were about 25 journalists who worked on this in the end. You need the time, the infrastructure to be able to produce this kind of investigation. The more we can raise awareness, the greater chance we have of survivors feeling like they're not alone and of spurring actual change.
So far, Motherless doesn't appear to have banned the so-called “sleep content,” although some related search terms or tags seem to have disappeared since the publication of CNN’s investigation. Meanwhile, other search terms still lead users to what appears to be drug-facilitated sexual assault content. The Zzz Telegram group has vanished from the Telegram chat list, but Telegram has not responded to CNN's questions about the disappearance.

Is ICE a reproductive health hazard?
 April 17, 2026 The “Toxic Legacy” of Operation Metro SurgeThis winter, in Minnesota and elsewhere around the country, ICE used tear gas on citizens. Now public health experts worry that these chemical weapons may be linked to reproductive problems. Yessenia Funes reports.BY YESSENIA FUNES TEAR GAS ON A STREET IN MINNEAPOLIS THIS WINTER. EVEN THOSE NOT PROTESTING WERE AFFECTED, RESIDENTS SAY. (PHOTO BY SCOTT OLSON/GETTY IMAGES.) Asha kept a bag ready throughout most of January and February. Inside, she packed bandages, gauze, water, saline, tourniquets, and general first aid. The 30-year-old works as a healthcare professional in Minneapolis, and when she’s off the clock, she responds to community emergencies as a street medic, mostly treating her neighbors who have been exposed to chemical weapons. On the day in January when federal officers shot and killed 31-year-old nurse Alex Pretti, she says, “I watched a lot of elderly people get tear-gassed.” And that wasn’t the first or the last time Asha, who is sharing only her first name to protect her identity, saw law enforcement attack her neighbors. Since the Trump administration’s Operation Metro Surge, which deployed 3,000 federal immigration agents to the Twin Cities, the emergencies have felt nonstop to Asha. The administration concluded its Minnesota incursion on Feb. 12, firing Homeland Security Secretary Kristi Noem weeks later, partly for her failure to manage the fallout in the state. Minneapolis is seeing fewer agents than in prior months, but people are still scared. And the whole city still feels the surge’s effects in their bodies—perhaps literally. Public health experts fear that ICE’s actions will leave a toxic legacy for communities across the country. In cities like Los Angeles, Portland, and Washington, D.C., independent analysts have raised concerns over federal officers’ indiscriminate deployment of chemical agents like tear gas or pepper spray—and not just on protesters. People are being exposed while stepping out for work or errands, or even sometimes at home. Researchers can’t easily study the long-term impacts of these weapons—there’s no ethical way to expose people to these chemicals in a controlled experiment—but what they do know paints an alarming portrait for public health, especially in women, people with uteruses, and children. Asha Hassan, an assistant professor of women’s health at the University of Minnesota Medical School (not to be confused with the street medic), began collecting data on reproductive health impacts in 2020 when the Black Lives Matter uprisings sprang up across the country and, with them, a police response that often involved tear gas. She had heard whispers of menstrual irregularities and miscarriages, but after looking at the available literature, she realized scientists had ignored some key population groups. “A lot of the research that we do have on tear gas is from the ’50s and ’60s,” Hassan explains. “It’s on mostly healthy men who are in a military setting. It really hasn’t been tested on women, children, people with chronic conditions, people with any sort of disability.” Studies have focused on “this particular type of body: a cis, straight man who is serving in the military and has the ability to be healthy.”  A PROTESTER IN LOS ANGELES FLUSHES A FELLOW DEMONSTRATOR’S EYES OUT AFTER EXPOSURE TO TEAR GAS. (PHOTO BY JON PUTMAN/ANADOLU VIA GETTY IMAGES After putting out a social media call to hear from those who had been exposed to chemical weapons like tear gas, she received more than 600 emails from all over the world in just a few weeks. In 2023, she published a paper that included more than 1,200 responses from people exposed in the U.S. between 2020 and 2021. The findings confirmed Hassan’s fears: Tear gas exposure was linked to negative reproductive health impacts for anyone of reproductive age. “Even after one exposure, we started to see some impact,” she says.
The more a person had been exposed, the more likely they were to face a number of issues: breast tenderness, spontaneous bleeding, and cramping. The study also found an above-average rate of miscarriages, but the sample size didn’t include enough pregnant participants to make a strong conclusion about tear gas’s effect. AN “OBJECTIVELY CHILLING” USE OF TEAR GASIn the decades after World War II, the majority of world leaders agreed to ban riot control agents during war as part of the Chemical Weapons Convention. (The U.S. government shares limited information on the chemicals that make up these weapons, but they can include chlorobenzylidene malononitrile and dibenzoxazepine, which can harm the respiratory system.) However, U.S. police are still allowed to use these weapons to protect public safety, explains Rohini Haar, a public health professor at U.C. Berkeley and medical adviser at Physicians for Human Rights. But that’s not what’s happening in the U.S. under Trump, Dr. Haar believes. “You’re not seeing that these weapons are used to quell any sort of riot or protect public safety,” Dr. Haar says, emphasizing that ICE agents have fired tear gas as protesters were walking away, not to disperse a crowd. “They’re actually harming public safety.” Dr. Haar has treated tear gas patients across the globe, including at the Aida Refugee Camp in the West Bank. There, Palestinian families have been exposed to periods of near-daily tear-gas use by Israeli soldiers. No one is safe—not people cooking dinner at home or children walking to school. “That’s happening now in the U.S., too,” Dr. Haar says. “The experience in Aida is kind of a warning.” Indeed, a federal judge ordered ICE to stop its use of tear gas in Oregon last month after the American Civil Liberties Union filed a lawsuit on behalf of protesters. In his filing, U.S. District Court Judge Michael Simon wrote, “Defendants’ conduct – physically harming protesters and journalists without prior dispersal warnings – is objectively chilling.” At least one additional case also focuses on the federal government’s recent use of chemical weapons in Portland. The Meteor reached out to Customs and Border Protection to understand its reasoning behind officers’ liberal use of tear gas. The agency did not comment, but Gregory Bovino, the ICE official who led the Minnesota operation and lost his job in January, has defended the use of chemical weapons as a favorable alternative to “lethal devices.” In Minneapolis, ICE agents have also deployed tear gas outside people’s apartments and buildings, where the chemicals can and do seep indoors. The weapons are most toxic in enclosed spaces. The day officers killed Pretti, Asha, the street medic, fled into an apartment building to catch a break. “The air inside was almost as bad as the air outside,” she recalls. “You were standing inside and coughing,” Asha says. Tear gas “was seeping into every apartment in that hallway.”  PEOPLE IN MINNEAPOLIS RUN FROM TEAR GAS—WHICH FEDERAL AGENTS USED WIDELY THE DAY THEY KILLED NURSE ALEX PRETTI. (PHOTO BY STEPHEN MATUREN/GETTY IMAGES) For those who aren’t familiar with the chemicals, stepping outside of one’s home can feel completely normal—until the stinging, dry stench hits, explains Minneapolis resident Slime Seamstress, a 31-year-old trans seamstress using their soon-to-be legal name. They were exposed to tear gas twice in January. They never attended a protest; exposure occurred instead during routine walks to pick up groceries or meet a friend. About a week later, they menstruated for more than 30 days straight. After three weeks of bleeding, they went to see their doctor, who suggested that the tear gas had caused the disruption. “That’s what scared me,” Seamstress says. “They said that it seemed serious.” Seamstress didn’t have the means to purchase more menstrual products after their supply ran out, so they sewed their own reusable pads with the fabrics they had at home. They can’t afford a gas mask, a $40-230+ product which has become essential for many Minnesotans, either. At the height of protests, Seamstress avoided leaving the house. “A HIGHLY TENSE SOCIAL AND PSYCHOLOGICAL SITUATION”Staying home isn’t an option for everyone. Timothy Monko, a former post-doctoral researcher at the University of Minnesota, has investigated these chemicals, contributing to a 2021 paper scrutinizing the safety of tear gas. The research’s takeaway was clear: “We should not be using it without actually understanding its effects,” Monko says. Those findings were enough to scare him and his wife: They may want more children in the future, so his wife carried her gas mask everywhere when ICE officers were regularly facing off against local community responders this winter. Monko isn’t the only researcher to make similar conclusions. Public health expert Patricia Huerta has heard accounts of irregular menstrual cycles and miscarriages following tear gas exposure in Chile. The associate professor of public health and medicine at Chile’s University of Concepción published a 2023 paper focused on the 2019 social uprisings there, where police used crowd control agents during protests. She’s unsure whether chemical exposure alone is to blame for people’s symptoms—or whether it acts in combination with the trauma people experience during these law enforcement confrontations. “It’s a highly tense social and psychological situation,” Huerta says. “It’s quite stressful. It’s the smoke. It’s the smell. It’s a policeman pointing at you with a shotgun that you don’t know will shoot a tear gas canister or a rubber bullet.” Every researcher interviewed for this story agrees that there is a lot regulators still don’t understand about the long-term impacts of exposure to various types of chemical agents, but that they know enough to say with confidence that ICE’s recent use of tear gas and pepper spray isn’t safe. In the meantime, Seamstress is anxious over their next menstrual cycle. Asha, the street medic, remains available should her neighbors need her again. She’ll respond to emergencies however she can as long as her community is under attack. “Through all this, we’re just trying to meet the needs of our community,” she says. “We’re just looking after our neighbors….If it’s dropping off groceries or helping people pay rent, then it’s that. If it’s helping people who have been tear-gassed or pepper-sprayed, then we do that. We’re just helping in whatever way we can.”  ABOUT YESSENIA FUNESYessenia Funes is an environmental journalist focused on uplifting the voices of society's most oppressed. She publishes a climate-justice newsletter called Possibilities, and has been published in The Guardian, The Verge, Yale Climate Connections, National Geographic, New York Magazine, and more.  ENJOY MORE OF THE METEOR Thanks for reading the Saturday Send. Got this from a friend? Don’t forget to sign up for The Meteor’s flagship newsletter, sent on Tuesdays and Thursdays. |

A Secret School for Girls
Inside the clandestine network of classrooms defying the Taliban in Afghanistan
By Jessie Williams
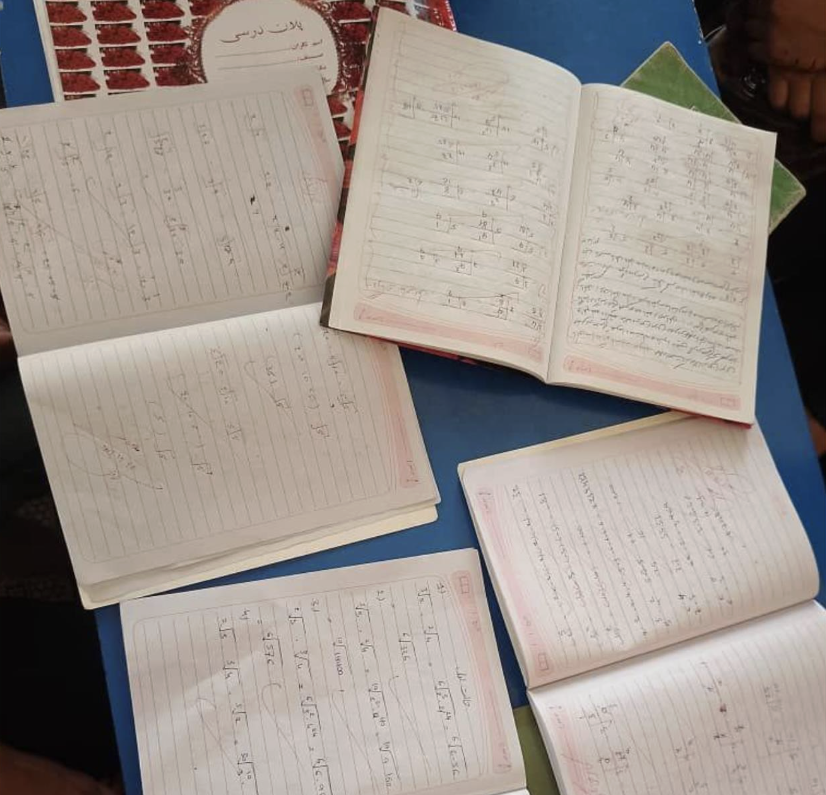
A group of teenage girls and young women gather in a nondescript room with pale walls, chatting and laughing. They have just finished their classes for the week and are about to head home. But they must leave one by one, so as not to draw any attention. If someone asks them where they have been, they say they were visiting the doctor. If they think someone might be on to them, the teachers move their classes to another person’s house. They leave their books at home. They must not be caught.
These girls live in Afghanistan, where education for girls beyond sixth grade is banned by the Taliban. They attend an underground girls’ school – one of five an Afghan NGO quietly runs across the country, with 28 teachers in different provinces providing free education to around 1,000 students, ranging in age from 13 to 45.
“I was very unhappy when the Taliban closed my school,” says Ada*, 15, who was in eighth grade when the Taliban returned to power on a hot summer day in 2021, following the withdrawal of U.S. and coalition forces. “I had depression.” The secret school she attends opened in the months afterward. “I feel better [now],” she says. “When I see the teachers and girls, I have power.”

As a new school year begins in Afghanistan, more than 2.2 million girls are currently out of school. But some of them are defying the ban. Over the past few years, classrooms have emerged in the shadows—cropping up in basements, living rooms and bedrooms around the country, away from the prying eyes of the Taliban, who have informants to catch people violating their strict codes. The schools use certain tactics to evade those informants, including staggering the timing of classes, so that some girls attend in the afternoon and some in the evening. If the girls think they’re being followed, they change their route. Madrassas, or religious schools, are still allowed, so if they are caught, they say they were going there.
The schools run by the NGO, which we can’t name for safety reasons, started through a network of trusted people in different communities. They cost about $60,000 to run each year, which a grant from the Frontline Women’s Fund, an initiative that supports women’s rights activists around the world, helps cover. One class was established and then another, and before long the network had blossomed into a web of clandestine schools, turning girls into what the Taliban fears most: educated women. “An educated woman changes the world,” says Laleh, 25, who teaches English at one of the schools. “An educated mother nurtures, trains, educates her kid. The kid changes the society.”
The Meteor spoke to the teachers and students over Zoom on the condition that we hide their identities. The stakes are high; if the Taliban ever found out about the schools, the teachers would be sent to prison, while the girls themselves could also face imprisonment and beatings. Despite the risks, the educators continue to teach. “When I was a girl, I studied chemistry. My father said ‘It's not safe to study.’ But I wanted to have a voice,” says Laleh. “When I teach the girls, they have the vocabulary to talk. It empowers me. When they learn, I think that I have done something in the world, that I didn't live a worthless life.”
Without education, she says, “our people don't even know how they should live and what their rights are…When half of our society is paralyzed, how can our country move forward?”
Since returning to power the Taliban has systematically eroded women’s and girls’ rights. Education for girls over sixth grade was the first to go, followed by barring women from university and nearly all forms of employment, then prohibiting them from playing sports, and even leaving the house without being completely covered and accompanied by a mahram or male guardian. The Taliban’s latest decree permits men to beat their wives as long as they don’t break any bones or leave open wounds.
The UN says that Afghan women are facing the most severe women’s rights crisis in the world, with many activists and human rights organizations calling it “gender apartheid”—a term meaning the systemic oppression, discrimination, and segregation of a specific group based on gender.
In January 2025, the International Criminal Court issued arrest warrants for the supreme leader and chief justice of the Taliban, accusing them of crimes against humanity for the persecution of women and girls. But nothing has been done to enforce the warrants. Even worse, the international community has begun to accept and normalize the Taliban as the de facto government, despite its draconian policies—like establishing embassies in Kabul, welcoming diplomats appointed by the Taliban, and inviting them to international summits.
Meanwhile, cuts to foreign aid budgets have meant dwindling humanitarian support for Afghanistan, and while the UN has continued its operations in the country, it faces major challenges—the main one being the ban on Afghan women entering UN premises, along with a 50 percent funding gap for UN work, which makes it difficult to provide services directly to women at a time when they desperately need it.
"Maybe they will arrest me and I go to jail. But I have to do this.”
Many Afghan women feel like the world has forgotten about them. Mariam, the 30-year-old executive director of the NGO that runs the schools, was a head teacher before the Taliban swept through the country. She says the international community should be doing more. “For five years girls and women can't go to school. It’s terrible. But nobody is doing anything,” she says. “Why aren’t the UN with us?”
Mariam says there are many women who are struggling financially now that they cannot work, and girls are being forced into early marriages. At the same time, recent clashes with Pakistan and war in neighboring Iran are exacerbating the already dire economic crisis.
For these girls, the school offers a glimmer of hope in an increasingly dark world, giving them the chance to forge their own futures. Bahar, a 19-year-old with a wide smile, was in 10th grade when the Taliban closed the schools. “When I come here I feel so excited,” she says, giggling. “I feel complete and confident.” Her favorite subjects are English and math, and one day she hopes to become a psychologist. “Education is very important to me. When girls use education, they can help their family.”
All of the girls’ families are supportive of them attending the classes, despite the dangers. “I feel happy because I improve my skills in this school,” says one student, Lama, 18. She especially loves art because it allows her to express her feelings, but wants to be a doctor when she’s older. “I want to help my people, always.”
Rehan, 21, a math teacher, says when she was her students’ age, “I had these opportunities as a student and I felt great. They should become what they want; I always teach them to become stronger.” Many of her students are vulnerable, she says, and so she makes sure to focus on their mental health. “When I come to class I ask them, ‘How was your day? How are you?’ Sometimes many of them don't have a good situation at home. First, I make sure they are safe, that they don't have any mental problems. Then I start to teach what I planned. I like to make the class a safer place for them.”
As the students and teachers talk, it becomes clear: These are much more than just schools. They also seem to be sanctuaries for women and girls to connect, laugh, and dream with friends. They are like a family, and Mariam, the head of the NGO, is the matriarch. She calls the students “my daughters” and sees supporting them as her responsibility. “It's a very big challenge,” she says. “We are afraid [of the Taliban finding out]. Maybe they will arrest me and I go to jail. But I have to do this.”
Despite the constant fear, they all still try to find joy – even if it’s fleeting. They dance and sing together when no one is looking. These girls are growing hope in the shadows; they’re creating cracks of light streaming through the darkness. “Sometimes we laugh, sometimes we cry,” says Mariam. “Maybe when the Taliban go, we will get our rights [back]. We want a new generation to feel peace.”
*All names in the piece have been changed to protect the subjects’ identity.

Jessie Williams is a freelance journalist focused on international affairs, humanitarian issues, and women’s rights, with work published in The Guardian, TIME Magazine, Foreign Policy, Al Jazeera, and more. She has reported from Syria, Lebanon, Iraq, and Ukraine, among other places.

We All Live in the Manosphere Now
Everyone’s talking about "Inside the Manosphere," but there’s one glaring omission.
By Nona Willis Aronowitz
Weeks after its release, everyone is still talking about Louis Theroux’s new documentary, "Inside the Manosphere." Theroux isn’t the first filmmaker to attempt to capture this subculture, but he’s arguably the most high-profile, applying his Michael Moore-esque style to these guys as he did to similarly odious groups like the Westboro Baptist Church and Scientologists. He tries to get inside the heads of wildly bigoted influencers like Harrison Sullivan (HSTickyTocky), Nicolas Kenn De Balinthazy (Sneako), Myron Gaines, and Justin Waller, focusing on how they profit off of marketing misogyny to young men.
Theroux, who has three sons of his own, mainly limits his scope to the influencers themselves and their throngs of young male fans, sons of the Millennial and Gen X women who ushered in a new era of feminist consciousness. Theroux makes it clear that we are now living through that movement’s backlash. And yet he seldom depicts the people who are most hurt by it: women.
It’s not that we don’t hear from women at all. Theroux briefly chats with the influencers’ women employees, wives, and girlfriends, whose remarks range from beatific assent (male domination is “how it’s supposed to be”) to resigned eye rolls (“Male audience. What can you expect?”). But Theroux never talks to them for more than a few minutes, and he almost never talks to them alone. The one time he manages to grab a few solo words with the woman who books guests on Myron Gaines’s show, Gaines immediately sends her a cease-and-desist text from the next room. The closest Theroux gets to a substantive interview with a woman is when he speaks with Harrison Sullivan’s mom, who supposedly “hates sexism.” Asked to comment on her son’s profession, she simply says, “Of course there’s things I don’t agree with.”

Maybe individual interviews with these particular women were impossible, but I was dying to know: Where are Sneako’s exes? Who are Waller’s former women employees or employers? Could we have heard from a girl who went to high school with Sullivan, or a woman who worked alongside Gaines when he was, ahem, a DHS agent? If Theroux really wanted to uncover their humanity, as he claims, that could have been a way to go.
The short interviews he does conduct with the wives and girlfriends often take on a distinctly paternalistic tone. Theroux harps on the one-sided monogamy many of these relationships have established; several of these men sleep with other women but expect their partners to remain “loyal.” It’s a valid data point about their chauvinism: As a practitioner of nonmonogamy myself, I can nevertheless concede that for more than a century, the jargon of “free love” has been twisted and manipulated by men to shame women into relationships they don’t want. But is polyamory the problem? Or just polyamory with misogynists?
And how, I was left wondering, do the women in these influencers’ lives feel about the rest of it? Why didn’t Theroux ask Waller’s partner, Kristen, about what she’s going to teach their two daughters, whose diapers Waller claims to never have changed? How did Gaines’s girlfriend, Angie, feel about being ordered to clean up their shared apartment before Theroux sees it? (Thank gawdess she’s no longer with him.) Does Sullivan’s mum worry about her son’s future wife, or her future grandchildren? When Theroux filmed Sneako taking selfies with a preteen boy—who jovially chants “Fuck the women!” and “All gays should die!”—did he give a passing thought to the girls or gays that go to school with him? Theroux interviews random male fans on the street about why they look up to Waller; perhaps he could have pulled aside a few women observing their fandom.

I found myself wanting to dispatch a girl gang to Theroux’s house, composed of regular women and girls who are exposed to this rhetoric on a daily basis. Like this 15-year-old girl who gave readers of The Guardian a glimpse into the “vile,” overtly misogynist content that social media feeds her, no matter how much she tries to steer the algorithm elsewhere. Or the girls in the classrooms of this educator, who reports that they’ve stopped raising their hands in class because “the social cost has become too high.”
And this isn’t just about one film. As Feminist points out, these glaring omissions mirror broader discussions about the “boy crisis” and the “male loneliness epidemic”—which, by the way, is not exclusively male; a recent Pew survey reported just as many women feeling lonely as men. These debates zero in on boys as victims of a patriarchal society, and they certainly are, but they’re not the only victims. A subset of these trend pieces blame feminism, not our society’s bedrock misogyny, which these influencers cynically enforce for their own gain. It feels ridiculous to even clarify this, but manosphere influencers are not akin to girlbosses; as Amanda Montei puts it, those women “may have run on white capitalist forms of exploitation, but they did not actively teach other women and girls to abuse, control, and dehumanize men, nor were they advocating for the end of men’s civil rights.” The women affected by this misogyny remain faceless and nameless while journalists give openly misogynist, racist, anti-Semitic influencers the royal treatment.
Not anymore. The Meteor will be rolling out a series on life and reality in this anti-feminist era, examining the backlash through the prism of women and girls who have to live through it. Stay tuned.

"The system is not set up for men to live their truth."
Heated Rivalry showed us what could be—but for gay men at the top levels of pro sports, that’s still just romantasy
When Heated Rivalry star Connor Storrie performed a portion of his Saturday Night Live opening monologue flanked by players from the men’s and women’s U.S national hockey teams, they formed a perfect pop culture panoptic. All at once, we had queer joy, the resolution of national sports beef, comedy, political commentary, and just a dash of pettiness for seasoning. While the moment bore the weight of so many things, that weight was shouldered entirely by sport, and where we as fans stand in our relationship to it.
For all the good that sports has given us, historically, it’s also been used as a tool of exclusion, with women, LGBTQ+ people, and athletes of color having to fight to exist in the courts, fields, and pitches they now enjoy. While there has been progress, it’s been slow and uneven. Over the last five years, 27 states have passed laws banning trans students from sports, and last summer, World Athletics mandated sex testing for women’s sporting categories—all in the name of “protecting” athletes from an amorphous queer menace.
At the same time, women’s sports have never been bigger, and incredible trans athletes, lesbians, non-binary Olympians, and bisexual baddies are all over our television screens.
But what about queer men? As Uncloseted Media wrote last year, there are “zero” gay or bisexual men actively competing at the highest professional levels of U.S. baseball, basketball, football, and hockey. That stat remains unchanged, but the success of Heated Rivalry and the current generation of queer athletes has many revisiting the age-old question: Why aren’t men coming out while active? When will we see hot hockey players kiss each other IRL? (I must note here that there have only ever been two hot men in hockey, Henrik Lundqvist and Martin St. Louis. They are both retired and, sadly, straight.)
“There’s so much performed masculinity that’s tied to men athletes,” explains Steve Granelli, Ph.D., a teaching professor of communications studies at Northeastern University. “It’s all rooted in this really toxic, very old understanding of gender roles.” That understanding is at the core of America’s Big Four—the MLB, NBA, NFL, and NHL—which have long played a major role in shaping our collective idea of what it means to be a man.
In the 150-year history of American professional sports leagues, only two men have come out while still actively playing. The first was the NBA’s Jason Collins in 2013, who announced he was gay in an article for Sports Illustrated, while signed to the Washington Wizards, and was widely supported by the league and the fans. (The loudest voice of dissent came from sports broadcaster Chris Broussard, who called homosexuality a sin on air.) Eight years later, the NFL defensive end Carl Nassib shared that he was gay in a social media post. In an interview with Good Morning America, Nassib said he was met with “nothing but love and support” by his teammates and his organization. He continued in the NFL until 2023, retiring as a Tampa Bay Buccaneer.
Since Collins, gay and bi men have slowly begun to take up space, just not while playing in the Big Four. Athletes across different sports have come out in retirement or after career-ending injuries, and it’s slightly more common to see queer men in a solo sport like tennis. Luke Prokop, an active player in the development league, the AHL, came out last summer. Earlier this year, inspired by Heated Rivalry, hockey player Jesse Korteum announced that he was gay and walked away from the sport when he was 17 because he didn’t think he would be accepted. In Japan’s B.League last year, Joshua Scott, an American basketball player who was a darling of the NCAA during his time at the University of Colorado, Boulder, came out publicly as bisexual.

Scott tells me that although he would “hear some off-putting stuff about what it was to be LGBTQ” in “a lot of locker rooms,” he never felt biphobia directed at him back in Colorado. That wasn’t entirely the case when he transitioned to the pros in Japan. “There was a season where, because there were different rumors tied to my sexuality, I received zero offers to play for a team,” he says. Not yet out of the closet, Scott felt he couldn’t combat the rumors publicly without doing more damage to his career. “The system is just not set up to help men be able to live their truth, and that starts at the youth level.”
Still, “being out and playing has been one of the most rewarding experiences,” he says. Scott announced that he was bisexual on social media, intentionally choosing to skirt Japanese media, which leans conservative. Since then, “I’ve gotten to almost have it all in a way I didn’t even think was possible four or five years ago.” Part of “having it all” has been success on the court, with Scott being one of his league’s top five players in rebounds and averaging a 62.4% field goal percentage. He also learned he “wasn’t alone,” he says. “There are a lot of people within the industry that are searching for a way to have both their truth and to be able to just do their sport.”
So far, that search has not borne fruit within the Big Four, where even straight players feel a pressure to hew to traditional roles. Granelli, who specializes in the study of sports culture and fandom, cites NFL player Caleb Williams, who is straight, as an example of just how little room men are given to express themselves outside the “acceptable” constraints of masculinity. “Williams comes into the NFL, and there’s such a focus on him painting his nails,” Granelli says. Williams, who is now a quarterback for the Bears, received a lot of negative feedback and questions for his personal style, which included themed nail sets; rapper Lil Wayne commented, “We just lost a playoff game to a [expletive] w purple nails we fkn suck” after the Packers lost to the Bears in January. “When men challenge the expected presentation of an athlete in any way, there is immediate backlash,” Granelli says. Fans eventually came around to Williams and his nails, but only after he’d put on a winning display of masculinity on the field.
Conversely, women athletes have created an entirely different space. “There’s a strong understanding [in women’s sports] that there’s a huge spectrum in terms of player sexuality,” says professional soccer player Tierna Davidson. A center back for Gotham FC, Davidson has been an out lesbian for her entire career and married her former teammate Alison Jahansouz in 2024. She says that women’s soccer specifically “has fostered a safe and welcoming environment for queer people”; sexual orientation was “never something I was worried about.” Davidson also gives some of the credit for this openness to fans. “If you look at the birth and nurturing of women's soccer in the U.S., there were so many strong, queer characters in that story,” she says. Women’s soccer “attracts fans that feel seen and represented, and it helps make our environment more open and welcoming. We don’t always get it right, but fans definitely see it and want to be part of it.”

On the men’s sports side, that fan-player relationship is just as key in determining how an athlete is received. “It only takes one moment, one small thing, for fans to feel a certain disconnect with a player and turn against him,” Granelli explains. “I mean, look at Josh Allen.” Allen, the beloved (straight) quarterback of the Buffalo Bills, had long been considered by fans as “one of us,” but upon his marriage to actress Hailee Steinfeld, a small subset of the Bills Mafia started calling him a sellout. “Dating someone from Hollywood is what makes him not like us?” Granelli, a lifelong Bills fan, groans. “He’s never been one of us! He’s 6’5” and has more talent than we’ll ever understand. But that’s all it takes for some people: One moment of not being able to identify with a player.”
Reimagining men’s sports to be more inclusive then becomes a chicken-and-egg quandary. Whose openness—an athlete’s, a fandom’s, or an organization’s—must come first to secure the openness of the other in a system that is built to be symbiotic? We are meant to see our most aspirational selves in athletes, and they, in turn, are made to feel secure and valued by our love. But too often the love of a fan does not extend to the fullness of an athlete’s persona, and if an athlete knows he cannot be fully himself and still receive that love, then why should he risk it? Women and trans athletes have more room to negotiate that risk because it is ever-present—they open their eyes in the morning, and that risk looms over them. But for men, who are shielded from bias by their athleticism and an assumed idea of masculinity, coming out means asking them to give up the one shred of safety they may feel they have.
Scott is hopeful that, eventually, that will all change. “There’s that adage that real men don’t cry,” he says. “But the beautiful part about sports is the passion, the anger, the disappointment, the tears and, yes, sometimes crying…[when I was closeted] I didn’t want to be exposed or have others think I was weak. But since coming out, I find myself stronger for walking in my truth.”

Lipstick, Selfies, and Prosthetic Legs
Gaza is home to the world’s largest group of child amputees. A photographer documents the lives of two of those children, who are still healing and waiting.
By Eman Mohammed
Layan’s first request after her surgeries was simple: She wanted to wear dresses again.
Before the bombing, she loved how fabric moved when she spun, how a skirt could flare and turn an ordinary hallway into a stage. After she lost both of her legs in an Israeli airstrike on her home in Gaza, dresses became a negotiation with balance, stitches, and pain. Learning to walk again meant relearning her body, figuring out how to trust it enough to stand inside the clothes she missed.
Layan is not the only child from Gaza learning to adapt to life-altering injuries. The United Nations has reported that Gaza is now home to the world's largest cohort of pediatric amputees per capita, with more than 4,000 children losing limbs since October 2023.
Most of those children remain in Gaza, with little hope of being evacuated to receive rehabilitation in a safe environment. Since October 2023, organizations like HEAL Palestine have facilitated secure passage for 62 children to the United States through medical visas, but in August 2025, those visas were suspended for Palestinian passport holders. Extensions quietly disappeared. When treatment ended, the Trump administration required their return. HEAL Palestine pledged not to send any Palestinian child back into an active genocide, and since then, those who could not remain in the U.S. have been placed in temporary housing in Cairo, waiting for borders to open, for stability to return, and for a future that does not yet exist.
Layan, 14, was one of the children who were granted medical evacuation to the United States through Heal Palestine. She arrived in Chicago in March 2024, and her host family has navigated lawyers, deadlines, and a system built to send her back before she was ready, fighting to keep her in the country while she relearns how to walk on both prosthetic legs. For now, her healing continues there, and she’s back in school. She still wants to go back to Gaza, not out of nostalgia, but because it is the only place that feels complete. Return remains blocked under Israeli restrictions.
Rozan, 13, understands interruption in a different way. After her evacuation for treatment, she was sent back to Egypt to wait for the borders to open. She lives with another family sponsored by HEAL Palestine, a mom and a three-year-old from Gaza. Her time in Cairo stretched from temporary to indefinite. Rozan lost her leg and seventeen members of her family in a single Israeli airstrike. The number sits in the room even when no one says it, but she doesn’t perform grief. She draws, studies, argues about outfits before school, and laughs when clay collapses in her hands on a pottery wheel, then tries again.
Neither girl fits the story people want from them. They are not symbols of unmitigated triumph. Their days revolve around prosthetic fittings, therapy schedules, visa deadlines, and the long logistics of survival. Healing is technical work. It takes money, translators, housing, doctors, tutors, and adults willing to build a net strong enough to hold children who have already fallen too far. That net exists because a community refused to let them disappear.
HEAL Palestine and the families around it function less like charity and more like extended kin. Apartments become shared recovery spaces. Older children teach new arrivals how to balance on unfamiliar legs. Caregivers trade information about clinics, schools, immigration rules. The girls grow inside that ecosystem of attention. Their resilience is not solitary, it is built collectively, reinforced by people who keep showing up.
In the afternoons, Rozan’s apartment fills with ordinary noise. A ball skids across the tile. Someone shouts. Someone laughs. Inside that chaos is the thing policy could not erase: children insisting on motion, and a community answering by making sure they never have to move alone.
Click on the images below to view the photo gallery.













Eman Mohammed is an award-winning Palestinian photojournalist from Gaza and Senior TED fellow. Her work has been featured in Le Monde, VICE, The Washington Post, The Atlantic and more.

She Fled Fear—and Found It Here
A woman who escaped danger in Afghanistan reflects on what life is like under ICE.
By Lima Halima-Khalil
I drop my three-year-old daughter off at library classes every morning. The library is two minutes from our home in Ashburn, Virginia. Each time, the same thought crosses my mind: Do I have my ID on me? Will my driver’s license be enough if I am stopped?
It is highly unlikely that I will encounter ICE on a two-minute drive to the library. Ashburn isn’t exactly an ICE hub. And yet my fear is constant, embodied, and real. And by the way, I am an American citizen.
I grew up believing America was a mighty country, one so powerful that the rest of the world stood intimidated by its strength. When I first came to the United States in 2006 for an education program from Afghanistan, a country still at war, the vastness of this place revealed itself not only in its size, but in the generosity of the people I met. After that, America became a place I always returned to. I have been part of the American education system since 2010, returning several times for various degrees. I’ve witnessed multiple presidential elections and participated in the most recent one as an American citizen myself.
But after all these years, one lesson about my new home stands out above the rest: This country is led, shaped, and sustained by fear. Outside this country, nations tremble at the military and economic power of the United States, but inside it, people live as though danger is always lurking.
Fear raises money and sustains campaigns. Fear keeps people glued to screens and locked into cycles of outrage. Fear sells guns, justifies surveillance, expands borders and prisons. Much of this fear is not grounded in lived reality but manufactured and amplified by politicians who rely on it to govern. Fear spills into kitchens, sidewalks, classrooms, and moments meant to be ordinary and human.

One of the most brutal tools in this ecosystem right now is ICE. Raids, detentions, and aggressive enforcement practices operate not simply as immigration policy, but as a mechanism of fear, reminding entire communities that their sense of belonging is fragile and conditional. ICE does not need to be everywhere to be effective. The possibility of its presence is enough.
This pervasive fear turns ordinary routines into sites of anxiety. I remember hesitating before offering to share our Thanksgiving meal with our nosy white neighbor, suddenly gripped by thoughts I never imagined I would carry. What if he calls the police on us and claims I was trying to poison him? What if kindness itself is misread as a threat, or hospitality as danger?
Afghans discovered how quickly they could become the “other,” regardless of their sacrifices, their loyalty, and their love for this country.
I recognize these impulses, because fear is not new to me. I lost my school, my home, my loved ones, and eventually my country because I wanted freedom from fear. Millions of Afghans had believed in democracy when America promised it to us for 20 years, until the United States withdrew from Afghanistan in 2021. We voted, we hoped, we worked alongside our American partners for a shared dream, but that freedom never came. In 2020, when my 24-year-old sister was killed by the Taliban in an IED attack in her car, that truth became undeniable. I understood then that Afghanistan was no longer safe, and that realization is what led me to come to the United States permanently.
When the Taliban returned to power in 2021, many Afghans, including members of my own family, were evacuated and brought into this country by our American allies. They arrived in this country under extremely harsh circumstances, believing they would find dignity, safety, and a chance to contribute. Instead, they discovered how quickly they could become the “other,” regardless of their sacrifices, their loyalty, and their love for this country.

I was reminded of this again in November of last year, after a man from Afghanistan, who had been trained and worked for the CIA in his country, shot two National Guard members in Washington, D.C. Overnight, an entire community began to be seen, once again, as terrorists. Instead of a careful and humane conversation about mental health, trauma, or resettlement failures, the Trump administration halted all immigration from Afghanistan and pledged to re-examine green card holders from 19 countries. Afghans, many of whom fled the very forces America claims to oppose, were once again forced to prove their innocence.
This is how fear functions. It identifies a moment of tragedy, strips it of context, assigns collective guilt, and converts pain into political currency.
For a long time, I believed that fear in this country belonged primarily to people of color, that violence was uneven, predictable, and racialized. Then the killings of Renée Good and later Alex Pretti shattered that belief. They forced a painful realization that in today’s America, no one is safe, not five-year-old Liam Conejo Ramos, not women citizens like Dulce Consuelo Díaz Morales and Nasra Ahmed, not elderly citizens like Scott Thao or longtime residents like Harjit Kaur, not white Americans, either.
Lately, I have felt fear settle into my own body in a way I did not expect. I realized I had been going to sleep holding fear, living with the same quiet dread that so many people here carry without ever naming it. One night, I caught myself thinking, almost with disbelief: Congratulations, Lima, you are an American now.
But it does not have to be this way. Americans deserve more than this constant weight of dread, clinging to them like a second skin. We deserve a country where fear is not the engine that keeps the system running, where safety is not promised to some by threatening others, and where power is not sustained by keeping people afraid.

Lima Halima-Khalil, Ph.D., is the program director of the “I Stand With You” campaign at ArtLords, a collective she co-founded, where she mobilizes global awareness against gender apartheid in Afghanistan. Her research explores youth resilience amid violence and displacement. Her writing has appeared in Foreign Policy, TRT World, and academic publications.